Welcome! ATRIO Health Plans presentation will begin shortly.






45 Slides1.80 MB
Welcome! ATRIO Health Plans presentation will begin shortly. Agent Name Licensed Sales Agent Agent Phone Agent Email Confidential – Not Intended for Distribution Value. Compassion.
Meet your local licensed sales agent Agent Name INSERT PHOTO Licensed Sales Agent Agent Phone # Agent Email I’m here to personally help you find the ATRIO Health Plan that’s the best fit for you. About Me: ‒ Service area: ‒ Certified to sell ATRIO Health Plans # of years ‒ Licensed in states ‒ Languages spoken: languages ‒ Community Involvement: Volunteer through organization name Confidential – Not Intended for Distribution Value. Compassion.
Agenda 1 Why ATRIO Health Plans 2 Understanding your Medicare Choices 3 Eligibility and enrollment 4 The Advantages of Medicare Advantage 5 Prescription Drug Coverage 6 2024 Medicare Advantage plan information 7 Agent assistance & Next Steps Confidential – Not Intended for Distribution Value. Compassion.
Why ATRIO Health Plans For 20 years, ATRIO has delivered high quality health insurance at a reasonable price, leveraged the talents of our people, and fostered deeper community connections. Confidential – Not Intended for Distribution Customer Service excellence Physician-led care coordination programs Access to quality care Educational resources Better patient outcomes Value. Compassion.
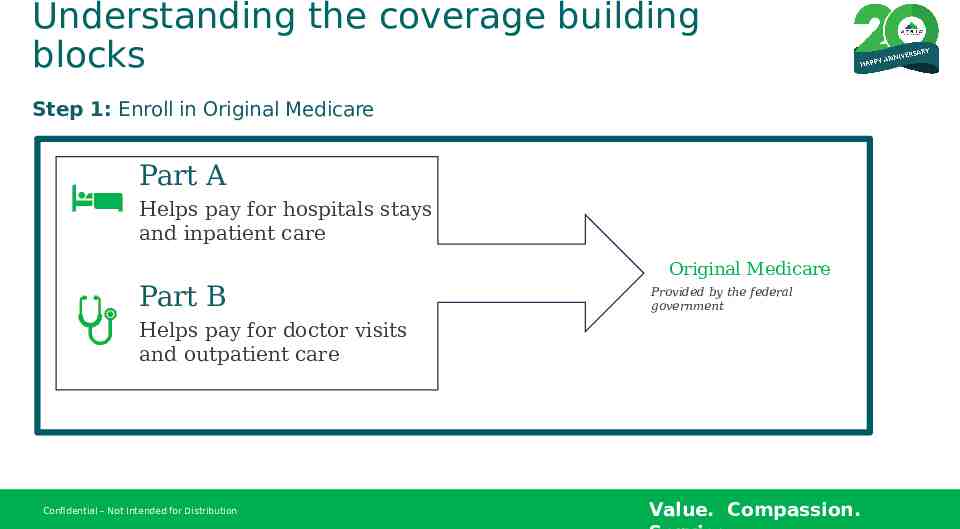
Understanding the coverage building blocks Step 1: Enroll in Original Medicare Part A Helps pay for hospitals stays and inpatient care Original Medicare Part B Provided by the federal government Helps pay for doctor visits and outpatient care Confidential – Not Intended for Distribution Value. Compassion.
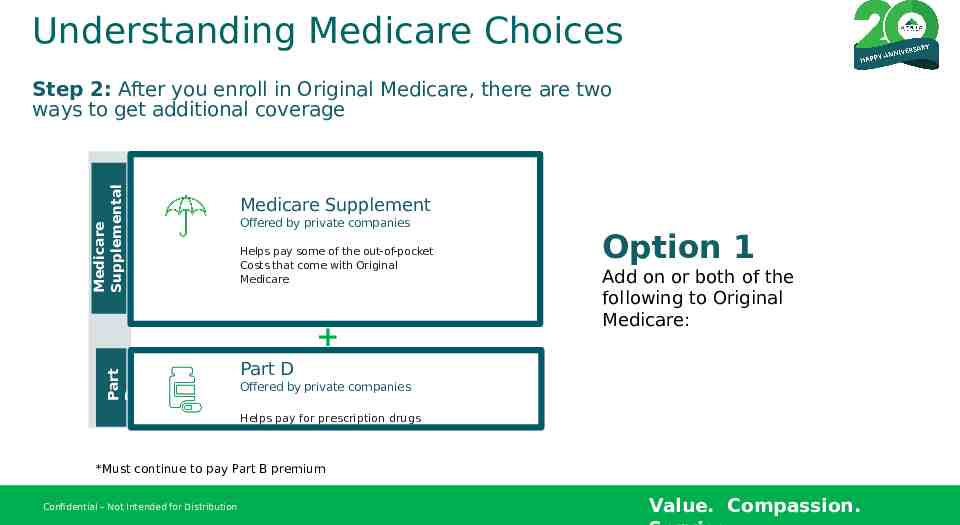
Understanding Medicare Choices Medicare Supplemental Step 2: After you enroll in Original Medicare, there are two ways to get additional coverage Medicare Supplement Offered by private companies Helps pay some of the out-of-pocket Costs that come with Original Medicare Part D Option 1 Add on or both of the following to Original Medicare: Part D Offered by private companies Helps pay for prescription drugs *Must continue to pay Part B premium Confidential – Not Intended for Distribution Value. Compassion.
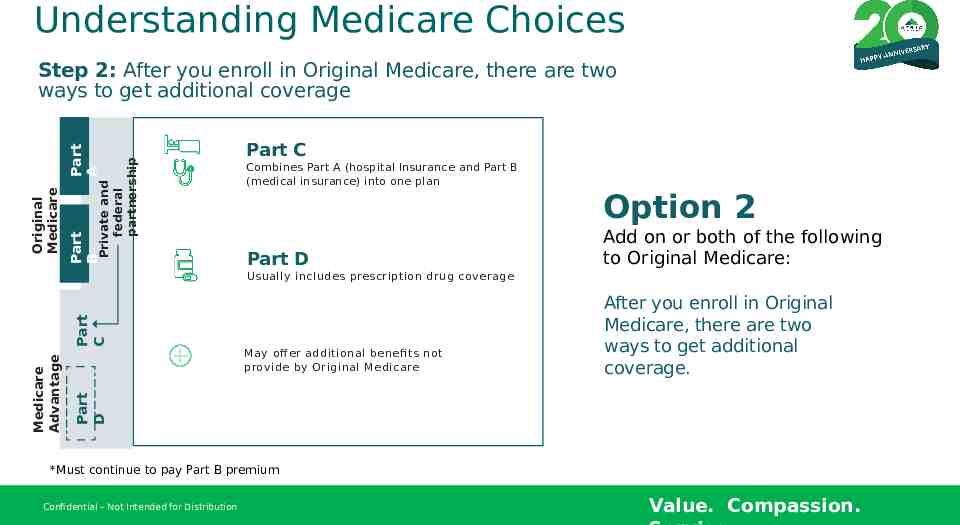
Understanding Medicare Choices Private and federal partnership Part B Original Medicare Part A Step 2: After you enroll in Original Medicare, there are two ways to get additional coverage Part C Combines Part A (hospital Insurance and Part B (medical insurance) into one plan Option 2 Part D Add on or both of the following to Original Medicare: May off er additional benefi ts not provide by Original Medicare After you enroll in Original Medicare, there are two ways to get additional coverage. Part D Medicare Advantage Part C Usually includes prescription drug coverage *Must continue to pay Part B premium Confidential – Not Intended for Distribution Value. Compassion.
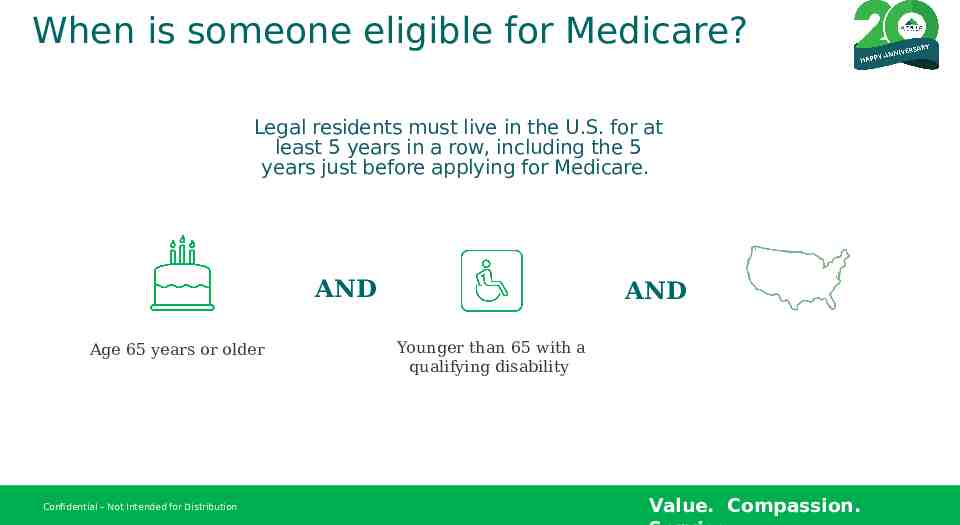
When is someone eligible for Medicare? Legal residents must live in the U.S. for at least 5 years in a row, including the 5 years just before applying for Medicare. AND Age 65 years or older Confidential – Not Intended for Distribution AND Younger than 65 with a qualifying disability Value. Compassion.
When can you enroll in a Medicare Advantage or prescription drug plan? Initial Enrollment Period Your Initial Enrollment Period (IEP) is 7 months long. It includes your 65th birthday month plus 3 months before, and the 3 months after. It begins and ends 1 month earlier if your birthday is on the first of the month. You may enroll in Part A, Part B or both. Confidential – Not Intended for Distribution You may also choose to join a Medicare Advantage plan (Part C) or a prescription Drug plan (Part D). Although you are not required to Enroll in Part D, there may be a penalty charged to your Part D premium if you didn’t enroll in prescription drug coverage when initially eligible for Medicare and didn’t have other creditable drug coverage to qualify for enrollment during a Special Enrollment Period. Or, you didn’t enroll in prescription drug coverage within 63 days of losing your creditable drug coverage. Value. Compassion.
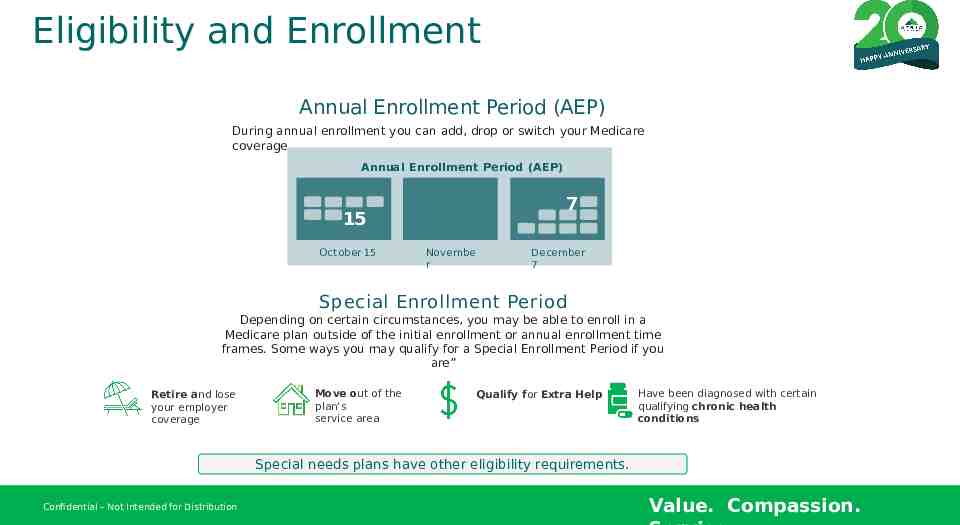
Eligibility and Enrollment Annual Enrollment Period (AEP) During annual enrollment you can add, drop or switch your Medicare coverage. Annual Enrollment Period (AEP) 15 October 15 1 5 Novembe r 7 1 5 December 7 Special Enrollment Period Depending on certain circumstances, you may be able to enroll in a Medicare plan outside of the initial enrollment or annual enrollment time frames. Some ways you may qualify for a Special Enrollment Period if you are” Retire and lose your employer coverage Move out of the plan’s service area Qualify for Extra Help Have been diagnosed with certain qualifying chronic health conditions Special needs plans have other eligibility requirements. Confidential – Not Intended for Distribution Value. Compassion.
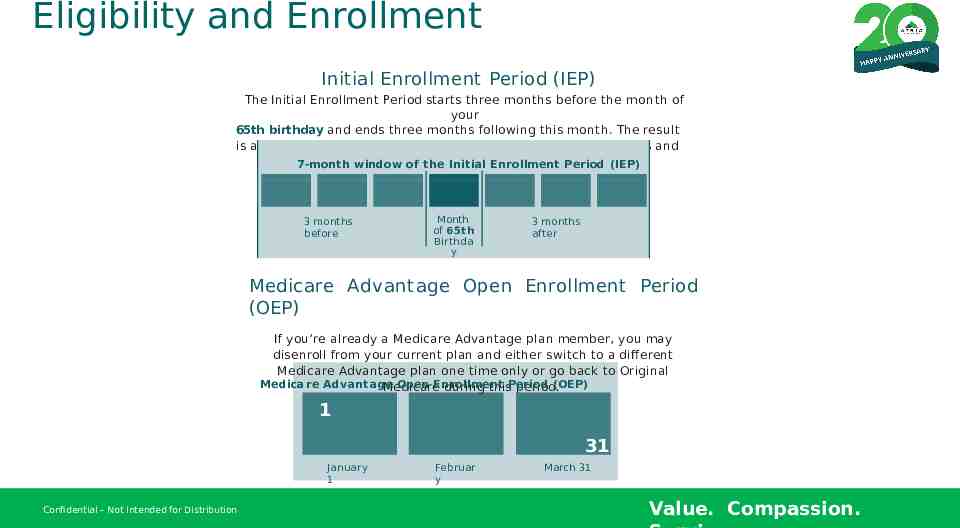
Eligibility and Enrollment Initial Enrollment Period (IEP) The Initial Enrollment Period starts three months before the month of your 65th birthday and ends three months following this month. The result is a 7-month period in which you can make your coverage choices and enroll. 7-month window of the Initial Enrollment Period (IEP) 3 months before Month of 65th Birthda y 3 months after Medicare Advantage Open Enrollment Period (OEP) If you’re already a Medicare Advantage plan member, you may disenroll from your current plan and either switch to a different Medicare Advantage plan one time only or go back to Original Medicare Advantage Open Enrollment (OEP) Medicare during thisPeriod period. 1 31 January 1 Confidential – Not Intended for Distribution Februar y March 31 Value. Compassion.
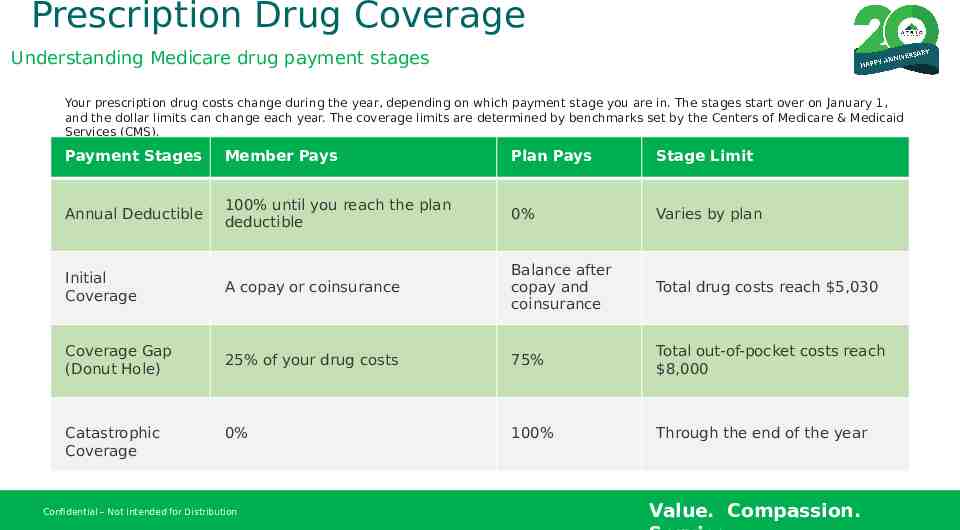
Prescription Drug Coverage Understanding Medicare drug payment stages Your prescription drug costs change during the year, depending on which payment stage you are in. The stages start over on January 1, and the dollar limits can change each year. The coverage limits are determined by benchmarks set by the Centers of Medicare & Medicaid Services (CMS). Payment Stages Member Pays Plan Pays Stage Limit Annual Deductible 100% until you reach the plan deductible 0% Varies by plan Initial Coverage A copay or coinsurance Balance after copay and coinsurance Total drug costs reach 5,030 Coverage Gap (Donut Hole) 25% of your drug costs 75% Total out-of-pocket costs reach 8,000 0% 100% Through the end of the year Catastrophic Coverage Confidential – Not Intended for Distribution Value. Compassion.
Prescription Drug Coverage What’s the difference between total drug costs and out-of-pocket costs? Total Drug Costs What you pay for prescription drugs each year, plus, what your plan pays. Does not include your premium. Out-of-Pocket Drug Costs The total amount you pay for prescription drugs, including your deductible and any discounts paid by drug manufactures while you are in the donut hole. Does not include what the plan pays or your premium. If you get Extra Help from Medicare with your Part D costs, ask your agent how the Part D deductible and coverage gap apply to you. Confidential – Not Intended for Distribution Value. Compassion.
Prescription Drug Coverage Pharmacy Network Flexibility Tier 1 – Preferred Generic Tier 2 – Generic Tier Tier 3 - Preferred Brand Freedom to choose preferred pharmacy Tier 4 - Non-Preferred Brand Tier 5 - Specialty Tier 6* - Select Care Drugs *Although this typically would be the highest cost tier, tier 6 is a 0 copay tier for certain important medications such as: Select Insulins Part D vaccines ACE-I/ARBs for treatment of high blood pressure or kidney protection Select antidiabetic drugs to treat diabetes Statins to treat high cholesterol You won’t pay more than 35, while you are in the Coverage Gap, for a one-month supply of each insulin product covered by our plan, no matter what cost-sharing tier it is on, even if you haven’t paid your deductible. Confidential – Not Intended for Distribution Save on one monthly copay on a 100-day prescription Save with mail service pharmacy Value. Compassion.
Prescription Drug Coverage Types of restrictions you might find on formulary drugs Prior Authorization (PA) – this is a request for approval in advance. Some drugs may require a prior authorization to make sure the drug is being used appropriately. Quantity Limits (QL) – certain drugs may have a specific quantity limit allowed to receive. Step Therapy (ST) – you may need to try other drugs first before we will approve the use of certain drugs to treat the same condition. Part B vs. Part D review – some drugs are covered as part of your medical Part B coverage, and others are covered under your Part D coverage. Confidential – Not Intended for Distribution Value. Compassion.
2024 Medicare Advantage Plan Information Confidential – Not Intended for Distribution Value. Compassion.
Why ATRIO Health Plans For 20 years, ATRIO Health Plans has been Oregon’s Local Medicare plan. PPO Plan Offerings allow you to seek medical providers across the U.S. at an Out-of-Network Cost. Confidential – Not Intended for Distribution Members have freedom to choose their preferred pharmacy. 0 copay on selected Insulin through our Tier 6 gives peace of mind and lower Rx costs. Rich Supplemental Benefits that go beyond Original Medicare. Flex Card: Dental, Fitness, OTC Meals Vision Telehealth Transportation Wearable devices Worldwide Emergency and Urgent Care Value. Compassion.
Member Experience What to expect when you enroll. As a new member, you will receive: Welcome Call As a new member, you will receive a call from our team, welcoming you to the ATRIO family. Quick Reference Guide This guide will provide some basic information, such as plan overview, accessing the member portal, preventive services and selecting a PCP. Welcome Packet This packet will include your specific plan information, provide information on scheduling appointments and more. Local Support Members will have access to local Customer Service Support by visiting one of our local offices. Mon-Fri, 8am-5pm. Confidential – Not Intended for Distribution Value. Compassion.
Member Experience Member ID Card This card will contain all your member information, including important contact numbers (i.e., customer service) should you have any questions. This will be important for you to carry on trips to the doctor’s office and to pick up prescriptions. Flex Card (Visa) Separately, you will also receive your ATRIO Flex Card in the mail, pre-loaded with allowances for your dental, gym, and OTC benefits (depending on your plan) Confidential – Not Intended for Distribution Value. Compassion.
Additional Resources for Medicare Beneficiaries ‒ Medicare Shoppers Guide ‒ Medicare Helpline ‒ Medicare.gov ‒ Social Security Administration ‒ Administration and Eldercare Locator ‒ State Resources Confidential – Not Intended for Distribution Value. Compassion.
2024 Enrollment Kit and Benefits We will Cover: ‒ 2024 ATRIO Plan Benefits ‒ Additional Benefits ‒ Star Ratings ‒ How to Enroll ‒ Plan Recap ‒ After you Enroll ‒ Notice of Nondiscrimination & Multi-Language WeResources will spend the next 30 minutes reviewing plan specific details and your enrollment options. [For virtual meetings we will share the approved 2024 Benefits at a Glance] Confidential – Not Intended for Distribution Value. Compassion.
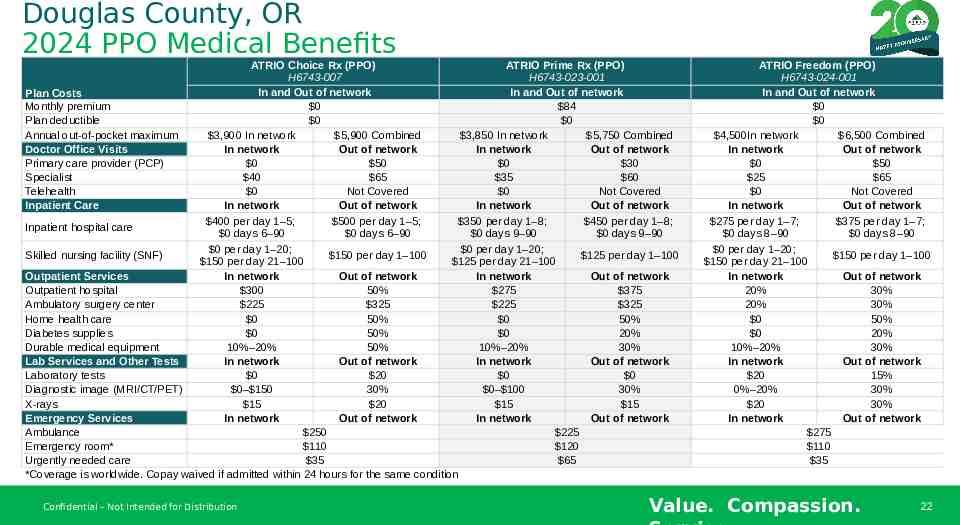
Douglas County, OR 2024 PPO Medical Benefits ATRIO Choice Rx (PPO) ATRIO Prime Rx (PPO) H6743-007 H6743-023-001 In and Out of network In and Out of network Plan Costs Monthly premium 0 84 Plan deductible 0 0 Annual out-of-pocket maximum 3,900 In network 5,900 Combined 3,850 In network 5,750 Combined Doctor Office Visits In network Out of network In network Out of network Primary care provider (PCP) 0 50 0 30 Specialist 40 65 35 60 Telehealth 0 Not Covered 0 Not Covered Inpatient Care In network Out of network In network Out of network 400 per day 1–5; 500 per day 1–5; 350 per day 1–8; 450 per day 1–8; Inpatient hospital care 0 days 6–90 0 days 6–90 0 days 9–90 0 days 9–90 0 per day 1–20; 0 per day 1–20; Skilled nursing facility (SNF) 150 per day 1–100 125 per day 1–100 150 per day 21–100 125 per day 21–100 Outpatient Services In network Out of network In network Out of network Outpatient hospital 300 50% 275 375 Ambulatory surgery center 225 325 225 325 Home health care 0 50% 0 50% Diabetes supplies 0 50% 0 20% Durable medical equipment 10%–20% 50% 10%–20% 30% Lab Services and Other Tests In network Out of network In network Out of network Laboratory tests 0 20 0 0 Diagnostic image (MRI/CT/PET) 0– 150 30% 0– 100 30% X-rays 15 20 15 15 Emergency Services In network Out of network In network Out of network Ambulance 250 225 Emergency room* 110 120 Urgently needed care 35 65 *Coverage is worldwide. Copay waived if admitted within 24 hours for the same condition Confidential – Not Intended for Distribution ATRIO Freedom (PPO) H6743-024-001 In and Out of network 0 0 4,500In network 6,500 Combined In network Out of network 0 50 25 65 0 Not Covered In network Out of network 275 per day 1–7; 375 per day 1–7; 0 days 8–90 0 days 8–90 0 per day 1–20; 150 per day 1–100 150 per day 21–100 In network Out of network 20% 30% 20% 30% 0 50% 0 20% 10%–20% 30% In network Out of network 20 15% 0%–20% 30% 20 30% In network Out of network 275 110 35 Value. Compassion. 22
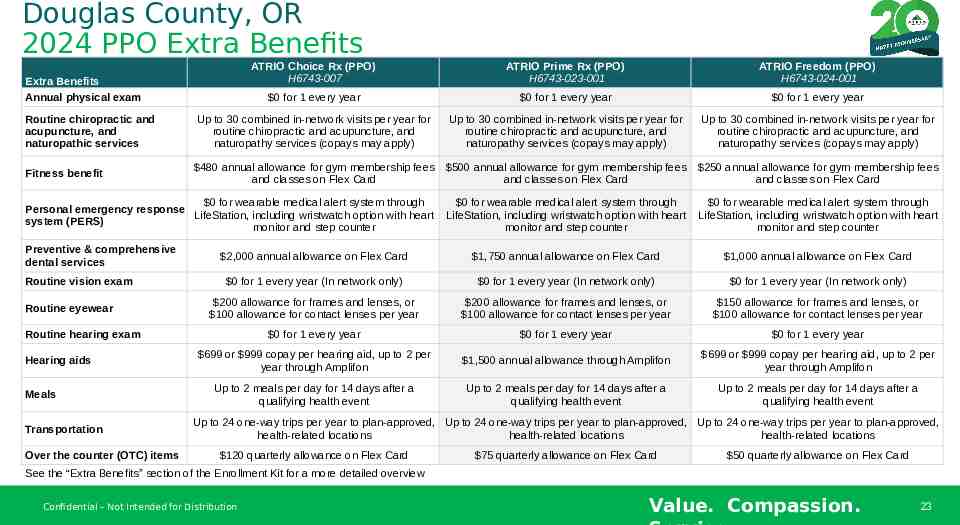
Douglas County, OR 2024 PPO Extra Benefits ATRIO Choice Rx (PPO) H6743-007 ATRIO Prime Rx (PPO) H6743-023-001 ATRIO Freedom (PPO) H6743-024-001 0 for 1 every year 0 for 1 every year 0 for 1 every year Routine chiropractic and acupuncture, and naturopathic services Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Fitness benefit 480 annual allowance for gym membership fees and classes on Flex Card 500 annual allowance for gym membership fees and classes on Flex Card 250 annual allowance for gym membership fees and classes on Flex Card 0 for wearable medical alert system through Personal emergency response LifeStation, including wristwatch option with heart system (PERS) monitor and step counter 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter 2,000 annual allowance on Flex Card 1,750 annual allowance on Flex Card 1,000 annual allowance on Flex Card 0 for 1 every year (In network only) 0 for 1 every year (In network only) 0 for 1 every year (In network only) 200 allowance for frames and lenses, or 100 allowance for contact lenses per year 200 allowance for frames and lenses, or 100 allowance for contact lenses per year 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 0 for 1 every year 0 for 1 every year 0 for 1 every year 699 or 999 copay per hearing aid, up to 2 per year through Amplifon 1,500 annual allowance through Amplifon 699 or 999 copay per hearing aid, up to 2 per year through Amplifon Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Extra Benefits Annual physical exam Preventive & comprehensive dental services Routine vision exam Routine eyewear Routine hearing exam Hearing aids Meals Transportation Over the counter (OTC) items Up to 24 one-way trips per year to plan-approved, Up to 24 one-way trips per year to plan-approved, Up to 24 one-way trips per year to plan-approved, health-related locations health-related locations health-related locations 120 quarterly allowance on Flex Card 75 quarterly allowance on Flex Card 50 quarterly allowance on Flex Card See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Confidential – Not Intended for Distribution Value. Compassion. 23
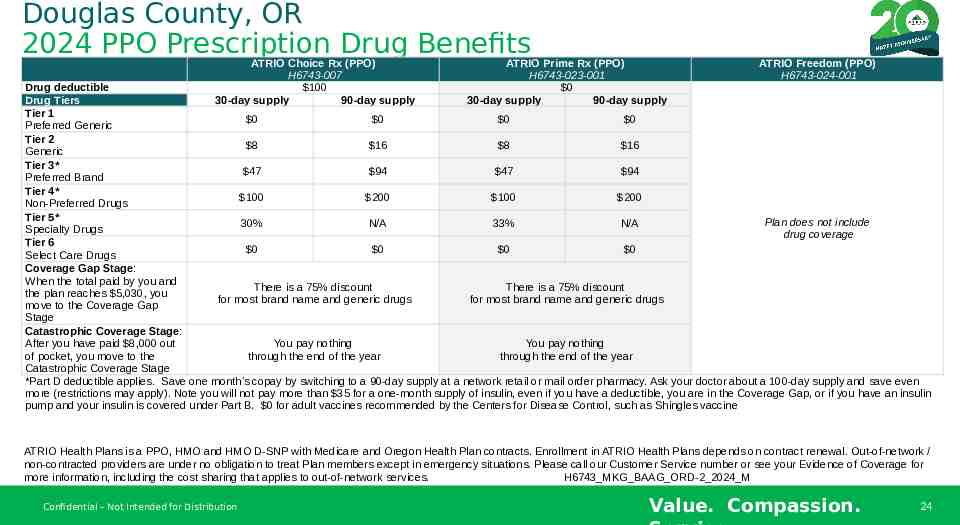
Douglas County, OR 2024 PPO Prescription Drug Benefits ATRIO Choice Rx (PPO) H6743-007 100 30-day supply 90-day supply ATRIO Prime Rx (PPO) H6743-023-001 0 30-day supply 90-day supply ATRIO Freedom (PPO) H6743-024-001 Drug deductible Drug Tiers Tier 1 0 0 0 0 Preferred Generic Tier 2 8 16 8 16 Generic Tier 3* 47 94 47 94 Preferred Brand Tier 4* 100 200 100 200 Non-Preferred Drugs Tier 5* Plan does not include 30% N/A 33% N/A Specialty Drugs drug coverage Tier 6 0 0 0 0 Select Care Drugs Coverage Gap Stage: When the total paid by you and There is a 75% discount There is a 75% discount the plan reaches 5,030, you for most brand name and generic drugs for most brand name and generic drugs move to the Coverage Gap Stage Catastrophic Coverage Stage: After you have paid 8,000 out You pay nothing You pay nothing of pocket, you move to the through the end of the year through the end of the year Catastrophic Coverage Stage *Part D deductible applies. Save one month’s copay by switching to a 90-day supply at a network retail or mail order pharmacy. Ask your doctor about a 100-day supply and save even more (restrictions may apply). Note you will not pay more than 35 for a one-month supply of insulin, even if you have a deductible, you are in the Coverage Gap, or if you have an insulin pump and your insulin is covered under Part B. 0 for adult vaccines recommended by the Centers for Disease Control, such as Shingles vaccine ATRIO Health Plans is a PPO, HMO and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on contract renewal. Out-of-network / non-contracted providers are under no obligation to treat Plan members except in emergency situations. Please call our Customer Service number or see your Evidence of Coverage for more information, including the cost sharing that applies to out-of-network services. H6743 MKG BAAG ORD-2 2024 M Confidential – Not Intended for Distribution Value. Compassion. 24
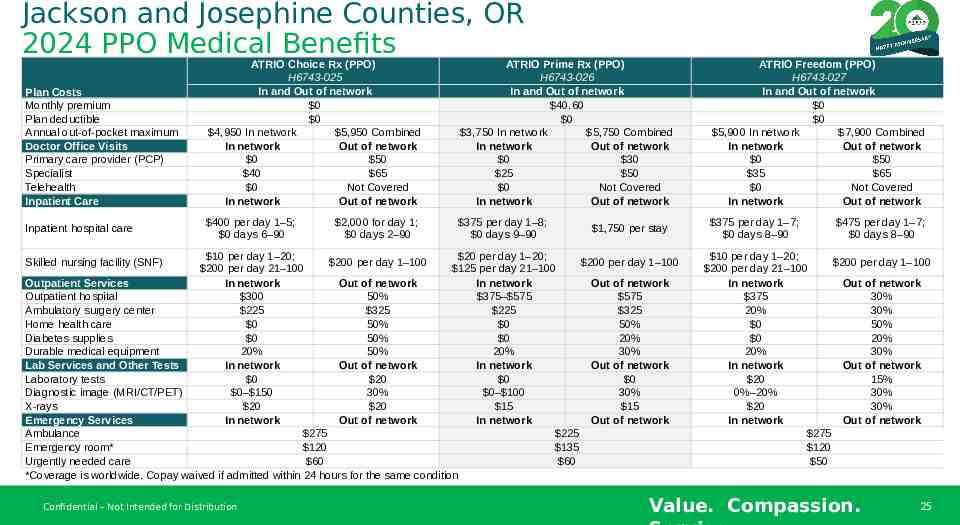
Jackson and Josephine Counties, OR 2024 PPO Medical Benefits Plan Costs Monthly premium Plan deductible Annual out-of-pocket maximum Doctor Office Visits Primary care provider (PCP) Specialist Telehealth Inpatient Care Inpatient hospital care ATRIO Choice Rx (PPO) H6743-025 In and Out of network 0 0 4,950 In network 5,950 Combined In network Out of network 0 50 40 65 0 Not Covered In network Out of network ATRIO Prime Rx (PPO) H6743-026 In and Out of network 40.60 0 3,750 In network 5,750 Combined In network Out of network 0 30 25 50 0 Not Covered In network Out of network ATRIO Freedom (PPO) H6743-027 In and Out of network 0 0 5,900 In network 7,900 Combined In network Out of network 0 50 35 65 0 Not Covered In network Out of network 400 per day 1–5; 0 days 6–90 375 per day 1–8; 0 days 9–90 375 per day 1–7; 0 days 8–90 2,000 for day 1; 0 days 2–90 1,750 per stay 10 per day 1–20; 20 per day 1–20; 200 per day 1–100 200 per day 1–100 200 per day 21–100 125 per day 21–100 Outpatient Services In network Out of network In network Out of network Outpatient hospital 300 50% 375– 575 575 Ambulatory surgery center 225 325 225 325 Home health care 0 50% 0 50% Diabetes supplies 0 50% 0 20% Durable medical equipment 20% 50% 20% 30% Lab Services and Other Tests In network Out of network In network Out of network Laboratory tests 0 20 0 0 Diagnostic image (MRI/CT/PET) 0– 150 30% 0– 100 30% X-rays 20 20 15 15 Emergency Services In network Out of network In network Out of network Ambulance 275 225 Emergency room* 120 135 Urgently needed care 60 60 *Coverage is worldwide. Copay waived if admitted within 24 hours for the same condition Skilled nursing facility (SNF) Confidential – Not Intended for Distribution 475 per day 1–7; 0 days 8–90 10 per day 1–20; 200 per day 1–100 200 per day 21–100 In network Out of network 375 30% 20% 30% 0 50% 0 20% 20% 30% In network Out of network 20 15% 0%–20% 30% 20 30% In network Out of network 275 120 50 Value. Compassion. 25
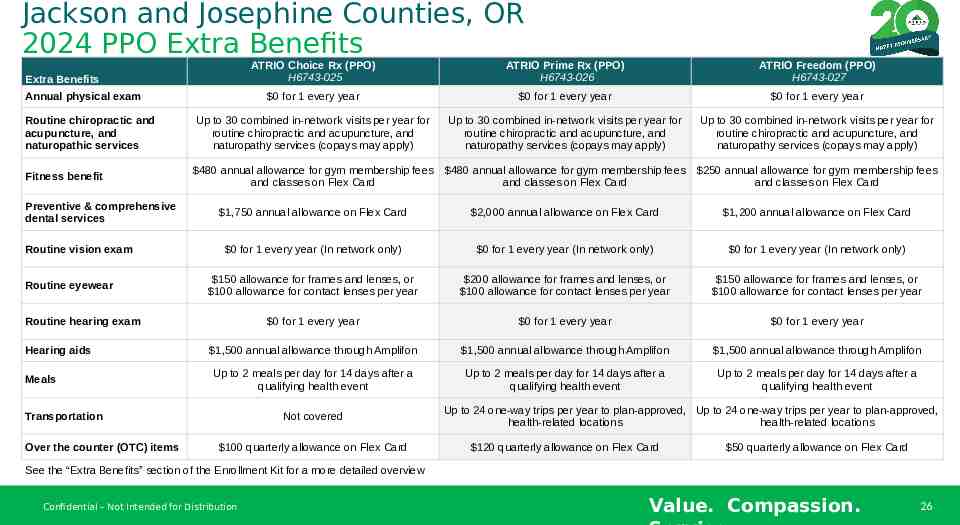
Jackson and Josephine Counties, OR 2024 PPO Extra Benefits ATRIO Choice Rx (PPO) H6743-025 ATRIO Prime Rx (PPO) H6743-026 ATRIO Freedom (PPO) H6743-027 0 for 1 every year 0 for 1 every year 0 for 1 every year Routine chiropractic and acupuncture, and naturopathic services Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Fitness benefit 480 annual allowance for gym membership fees and classes on Flex Card 480 annual allowance for gym membership fees and classes on Flex Card 250 annual allowance for gym membership fees and classes on Flex Card 1,750 annual allowance on Flex Card 2,000 annual allowance on Flex Card 1,200 annual allowance on Flex Card 0 for 1 every year (In network only) 0 for 1 every year (In network only) 0 for 1 every year (In network only) 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 200 allowance for frames and lenses, or 100 allowance for contact lenses per year 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 0 for 1 every year 0 for 1 every year 0 for 1 every year 1,500 annual allowance through Amplifon 1,500 annual allowance through Amplifon 1,500 annual allowance through Amplifon Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Extra Benefits Annual physical exam Preventive & comprehensive dental services Routine vision exam Routine eyewear Routine hearing exam Hearing aids Meals Transportation Over the counter (OTC) items Not covered 100 quarterly allowance on Flex Card Up to 24 one-way trips per year to plan-approved, Up to 24 one-way trips per year to plan-approved, health-related locations health-related locations 120 quarterly allowance on Flex Card 50 quarterly allowance on Flex Card See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Confidential – Not Intended for Distribution Value. Compassion. 26
Jackson and Josephine Counties, OR 2024 PPO Prescription Drug Benefits ATRIO Choice Rx (PPO) H6743-025 200 30-day supply 90-day supply ATRIO Prime Rx (PPO) H6743-026 0 30-day supply 90-day supply ATRIO Freedom (PPO) H6743-027 Drug deductible Drug Tiers Tier 1 0 0 0 0 Preferred Generic Tier 2 8 16 8 16 Generic Tier 3* 47 94 47 94 Preferred Brand Tier 4* 100 200 100 200 Non-Preferred Drugs Tier 5* Plan does not include 30% N/A 33% N/A Specialty Drugs drug coverage Tier 6 0 0 0 0 Select Care Drugs Coverage Gap Stage: When the total paid by you and There is a 75% discount There is a 75% discount the plan reaches 5,030, you for most brand name and generic drugs for most brand name and generic drugs move to the Coverage Gap Stage Catastrophic Coverage Stage: After you have paid 8,000 out You pay nothing You pay nothing of pocket, you move to the through the end of the year through the end of the year Catastrophic Coverage Stage *Part D deductible applies. Save one month’s copay by switching to a 90-day supply at a network retail or mail order pharmacy. Ask your doctor about a 100-day supply and save even more (restrictions may apply). Note you will not pay more than 35 for a one-month supply of insulin, even if you have a deductible, you are in the Coverage Gap, or if you have an insulin pump and your insulin is covered under Part B. 0 for adult vaccines recommended by the Centers for Disease Control, such as Shingles vaccine ATRIO Health Plans is a PPO, HMO and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on contract renewal. Out-of-network / non-contracted providers are under no obligation to treat Plan members except in emergency situations. Please call our Customer Service number or see your Evidence of Coverage for more information, including the cost sharing that applies to out-of-network services. H6743 MKG BAAG ORJAJO-2 2024 M Confidential – Not Intended for Distribution Value. Compassion. 27
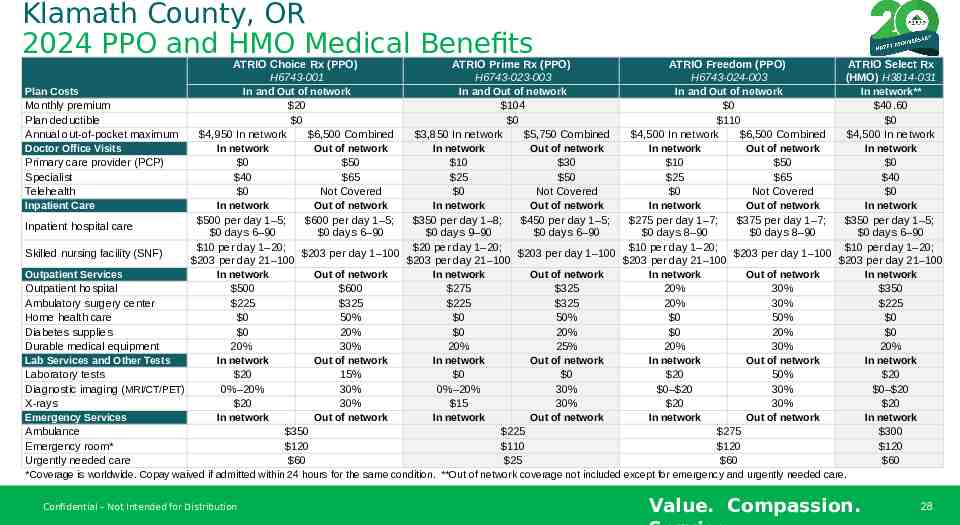
Klamath County, OR 2024 PPO and HMO Medical Benefits ATRIO Choice Rx (PPO) ATRIO Prime Rx (PPO) ATRIO Freedom (PPO) ATRIO Select Rx H6743-001 H6743-023-003 H6743-024-003 (HMO) H3814-031 In and Out of network In and Out of network In and Out of network In network** Plan Costs Monthly premium 20 104 0 40.60 Plan deductible 0 0 110 0 Annual out-of-pocket maximum 4,950 In network 6,500 Combined 3,850 In network 5,750 Combined 4,500 In network 6,500 Combined 4,500 In network Doctor Office Visits In network Out of network In network Out of network In network Out of network In network Primary care provider (PCP) 0 50 10 30 10 50 0 Specialist 40 65 25 50 25 65 40 Telehealth 0 Not Covered 0 Not Covered 0 Not Covered 0 Inpatient Care In network Out of network In network Out of network In network Out of network In network 500 per day 1–5; 600 per day 1–5; 350 per day 1–8; 450 per day 1–5; 275 per day 1–7; 375 per day 1–7; 350 per day 1–5; Inpatient hospital care 0 days 6–90 0 days 6–90 0 days 9–90 0 days 6–90 0 days 8–90 0 days 8–90 0 days 6–90 10 per day 1–20; 20 per day 1–20; 10 per day 1–20; 10 per day 1–20; Skilled nursing facility (SNF) 203 per day 1–100 203 per day 1–100 203 per day 1–100 203 per day 21–100 203 per day 21–100 203 per day 21–100 203 per day 21–100 Outpatient Services In network Out of network In network Out of network In network Out of network In network Outpatient hospital 500 600 275 325 20% 30% 350 Ambulatory surgery center 225 325 225 325 20% 30% 225 Home health care 0 50% 0 50% 0 50% 0 Diabetes supplies 0 20% 0 20% 0 20% 0 Durable medical equipment 20% 30% 20% 25% 20% 30% 20% Lab Services and Other Tests In network Out of network In network Out of network In network Out of network In network Laboratory tests 20 15% 0 0 20 50% 20 Diagnostic imaging (MRI/CT/PET) 0%–20% 30% 0%–20% 30% 0– 20 30% 0– 20 X-rays 20 30% 15 30% 20 30% 20 Emergency Services In network Out of network In network Out of network In network Out of network In network Ambulance 350 225 275 300 Emergency room* 120 110 120 120 Urgently needed care 60 25 60 60 *Coverage is worldwide. Copay waived if admitted within 24 hours for the same condition. **Out of network coverage not included except for emergency and urgently needed care. Confidential – Not Intended for Distribution Value. Compassion. 28
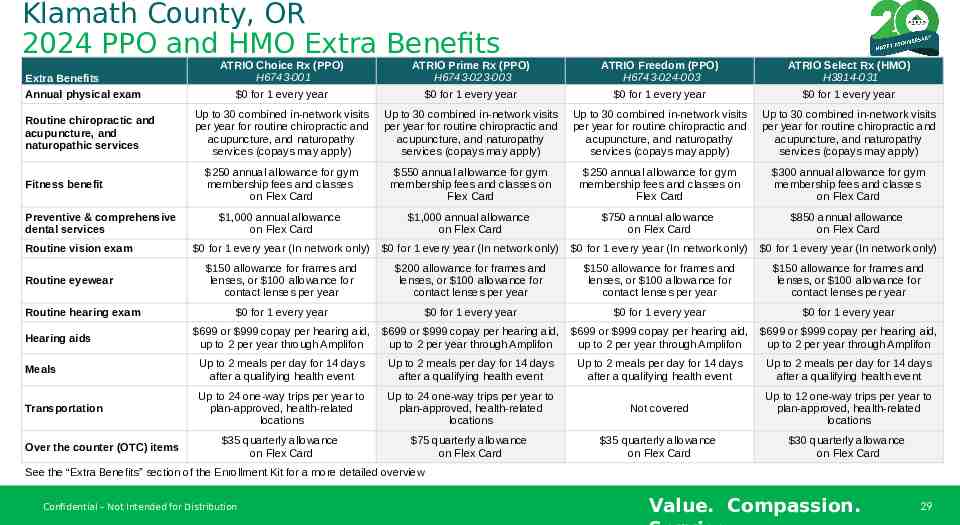
Klamath County, OR 2024 PPO and HMO Extra Benefits ATRIO Choice Rx (PPO) H6743-001 ATRIO Prime Rx (PPO) H6743-023-003 ATRIO Freedom (PPO) H6743-024-003 ATRIO Select Rx (HMO) H3814-031 0 for 1 every year 0 for 1 every year 0 for 1 every year 0 for 1 every year Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) 250 annual allowance for gym membership fees and classes on Flex Card 550 annual allowance for gym membership fees and classes on Flex Card 250 annual allowance for gym membership fees and classes on Flex Card 300 annual allowance for gym membership fees and classes on Flex Card 1,000 annual allowance on Flex Card 1,000 annual allowance on Flex Card 750 annual allowance on Flex Card 850 annual allowance on Flex Card 0 for 1 every year (In network only) 0 for 1 every year (In network only) 0 for 1 every year (In network only) 0 for 1 every year (In network only) 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 200 allowance for frames and lenses, or 100 allowance for contact lenses per year 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 0 for 1 every year 0 for 1 every year 0 for 1 every year 0 for 1 every year 699 or 999 copay per hearing aid, up to 2 per year through Amplifon 699 or 999 copay per hearing aid, up to 2 per year through Amplifon 699 or 999 copay per hearing aid, up to 2 per year through Amplifon 699 or 999 copay per hearing aid, up to 2 per year through Amplifon Meals Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Transportation Up to 24 one-way trips per year to plan-approved, health-related locations Up to 24 one-way trips per year to plan-approved, health-related locations Not covered Up to 12 one-way trips per year to plan-approved, health-related locations 35 quarterly allowance on Flex Card 75 quarterly allowance on Flex Card 35 quarterly allowance on Flex Card 30 quarterly allowance on Flex Card Extra Benefits Annual physical exam Routine chiropractic and acupuncture, and naturopathic services Fitness benefit Preventive & comprehensive dental services Routine vision exam Routine eyewear Routine hearing exam Hearing aids Over the counter (OTC) items See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Confidential – Not Intended for Distribution Value. Compassion. 29
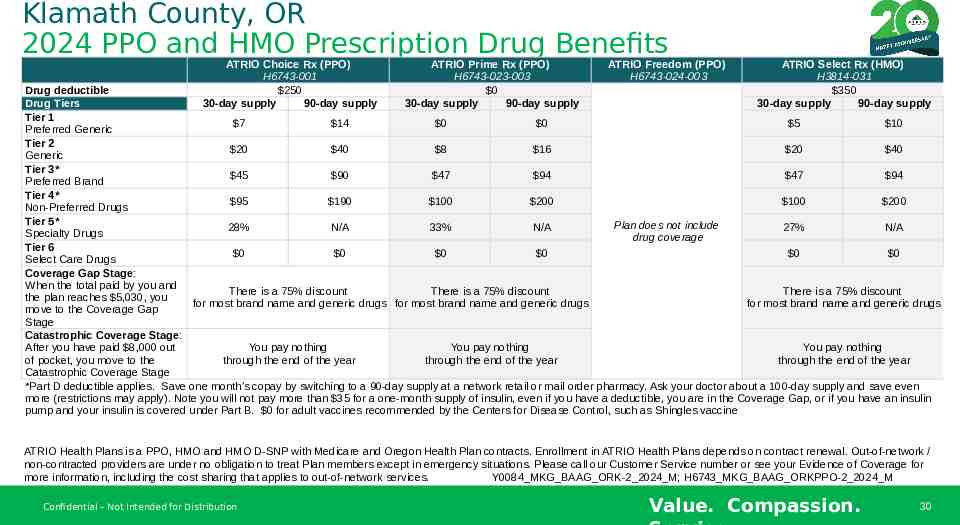
Klamath County, OR 2024 PPO and HMO Prescription Drug Benefits ATRIO Choice Rx (PPO) H6743-001 250 30-day supply 90-day supply ATRIO Prime Rx (PPO) H6743-023-003 0 30-day supply 90-day supply ATRIO Freedom (PPO) H6743-024-003 ATRIO Select Rx (HMO) H3814-031 350 30-day supply 90-day supply Drug deductible Drug Tiers Tier 1 7 14 0 0 5 10 Preferred Generic Tier 2 20 40 8 16 20 40 Generic Tier 3* 45 90 47 94 47 94 Preferred Brand Tier 4* 95 190 100 200 100 200 Non-Preferred Drugs Tier 5* Plan does not include 28% N/A 33% N/A 27% N/A Specialty Drugs drug coverage Tier 6 0 0 0 0 0 0 Select Care Drugs Coverage Gap Stage: When the total paid by you and There is a 75% discount There is a 75% discount There is a 75% discount the plan reaches 5,030, you for most brand name and generic drugs for most brand name and generic drugs for most brand name and generic drugs move to the Coverage Gap Stage Catastrophic Coverage Stage: After you have paid 8,000 out You pay nothing You pay nothing You pay nothing of pocket, you move to the through the end of the year through the end of the year through the end of the year Catastrophic Coverage Stage *Part D deductible applies. Save one month’s copay by switching to a 90-day supply at a network retail or mail order pharmacy. Ask your doctor about a 100-day supply and save even more (restrictions may apply). Note you will not pay more than 35 for a one-month supply of insulin, even if you have a deductible, you are in the Coverage Gap, or if you have an insulin pump and your insulin is covered under Part B. 0 for adult vaccines recommended by the Centers for Disease Control, such as Shingles vaccine ATRIO Health Plans is a PPO, HMO and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on contract renewal. Out-of-network / non-contracted providers are under no obligation to treat Plan members except in emergency situations. Please call our Customer Service number or see your Evidence of Coverage for more information, including the cost sharing that applies to out-of-network services. Y0084 MKG BAAG ORK-2 2024 M; H6743 MKG BAAG ORKPPO-2 2024 M Confidential – Not Intended for Distribution Value. Compassion. 30
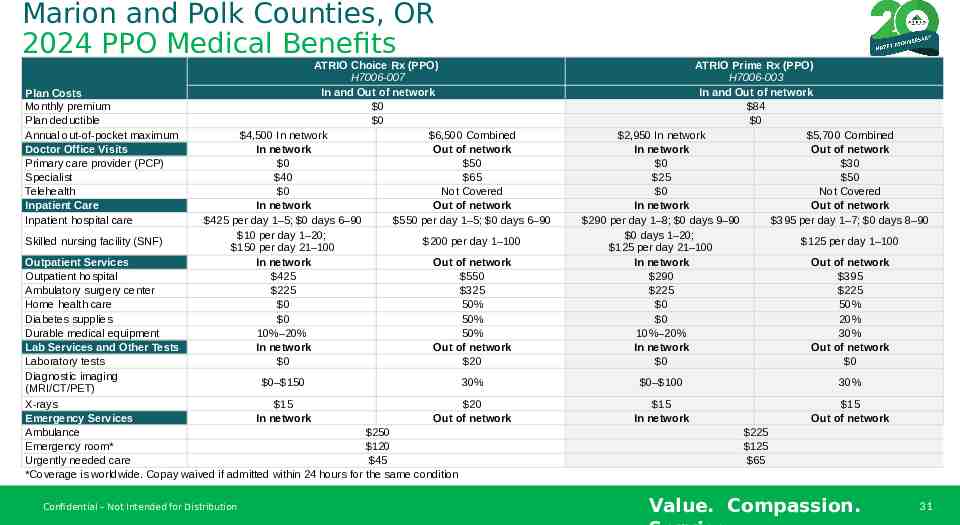
Marion and Polk Counties, OR 2024 PPO Medical Benefits Plan Costs Monthly premium Plan deductible Annual out-of-pocket maximum Doctor Office Visits Primary care provider (PCP) Specialist Telehealth Inpatient Care Inpatient hospital care Skilled nursing facility (SNF) ATRIO Choice Rx (PPO) H7006-007 In and Out of network 0 0 4,500 In network 6,500 Combined In network Out of network 0 50 40 65 0 Not Covered In network Out of network 425 per day 1–5; 0 days 6–90 550 per day 1–5; 0 days 6–90 10 per day 1–20; 200 per day 1–100 150 per day 21–100 In network Out of network 425 550 225 325 0 50% 0 50% 10%–20% 50% In network Out of network 0 20 Outpatient Services Outpatient hospital Ambulatory surgery center Home health care Diabetes supplies Durable medical equipment Lab Services and Other Tests Laboratory tests Diagnostic imaging 0– 150 30% (MRI/CT/PET) X-rays 15 20 Emergency Services In network Out of network Ambulance 250 Emergency room* 120 Urgently needed care 45 *Coverage is worldwide. Copay waived if admitted within 24 hours for the same condition Confidential – Not Intended for Distribution ATRIO Prime Rx (PPO) H7006-003 In and Out of network 84 0 2,950 In network 5,700 Combined In network Out of network 0 30 25 50 0 Not Covered In network Out of network 290 per day 1–8; 0 days 9–90 395 per day 1–7; 0 days 8–90 0 days 1–20; 125 per day 1–100 125 per day 21–100 In network Out of network 290 395 225 225 0 50% 0 20% 10%–20% 30% In network Out of network 0 0 0– 100 30% 15 In network 15 Out of network 225 125 65 Value. Compassion. 31
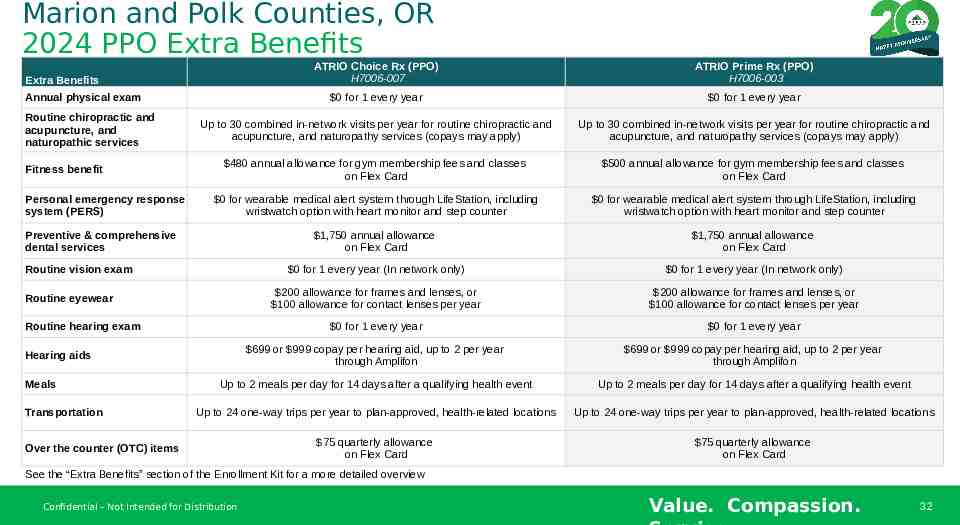
Marion and Polk Counties, OR 2024 PPO Extra Benefits ATRIO Choice Rx (PPO) H7006-007 ATRIO Prime Rx (PPO) H7006-003 0 for 1 every year 0 for 1 every year Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays may apply) 480 annual allowance for gym membership fees and classes on Flex Card 500 annual allowance for gym membership fees and classes on Flex Card 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter 1,750 annual allowance on Flex Card 1,750 annual allowance on Flex Card 0 for 1 every year (In network only) 0 for 1 every year (In network only) 200 allowance for frames and lenses, or 100 allowance for contact lenses per year 200 allowance for frames and lenses, or 100 allowance for contact lenses per year 0 for 1 every year 0 for 1 every year 699 or 999 copay per hearing aid, up to 2 per year through Amplifon 699 or 999 copay per hearing aid, up to 2 per year through Amplifon Up to 2 meals per day for 14 days after a qualifying health event Up to 2 meals per day for 14 days after a qualifying health event Up to 24 one-way trips per year to plan-approved, health-related locations Up to 24 one-way trips per year to plan-approved, health-related locations 75 quarterly allowance on Flex Card 75 quarterly allowance on Flex Card Extra Benefits Annual physical exam Routine chiropractic and acupuncture, and naturopathic services Fitness benefit Personal emergency response system (PERS) Preventive & comprehensive dental services Routine vision exam Routine eyewear Routine hearing exam Hearing aids Meals Transportation Over the counter (OTC) items See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Confidential – Not Intended for Distribution Value. Compassion. 32
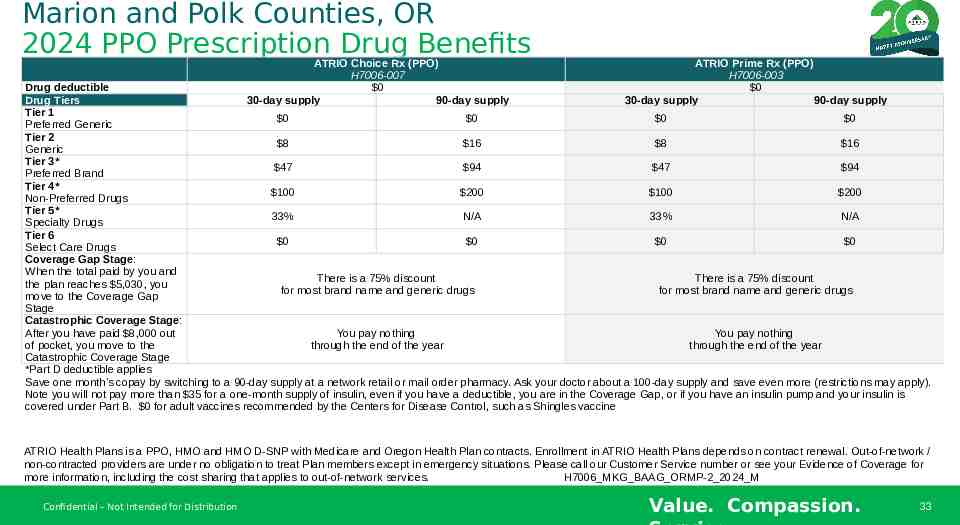
Marion and Polk Counties, OR 2024 PPO Prescription Drug Benefits ATRIO Choice Rx (PPO) H7006-007 0 30-day supply 90-day supply ATRIO Prime Rx (PPO) H7006-003 0 30-day supply 90-day supply Drug deductible Drug Tiers Tier 1 0 0 0 0 Preferred Generic Tier 2 8 16 8 16 Generic Tier 3* 47 94 47 94 Preferred Brand Tier 4* 100 200 100 200 Non-Preferred Drugs Tier 5* 33% N/A 33% N/A Specialty Drugs Tier 6 0 0 0 0 Select Care Drugs Coverage Gap Stage: When the total paid by you and There is a 75% discount There is a 75% discount the plan reaches 5,030, you for most brand name and generic drugs for most brand name and generic drugs move to the Coverage Gap Stage Catastrophic Coverage Stage: After you have paid 8,000 out You pay nothing You pay nothing of pocket, you move to the through the end of the year through the end of the year Catastrophic Coverage Stage *Part D deductible applies Save one month’s copay by switching to a 90-day supply at a network retail or mail order pharmacy. Ask your doctor about a 100-day supply and save even more (restrictions may apply). Note you will not pay more than 35 for a one-month supply of insulin, even if you have a deductible, you are in the Coverage Gap, or if you have an insulin pump and your insulin is covered under Part B. 0 for adult vaccines recommended by the Centers for Disease Control, such as Shingles vaccine ATRIO Health Plans is a PPO, HMO and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on contract renewal. Out-of-network / non-contracted providers are under no obligation to treat Plan members except in emergency situations. Please call our Customer Service number or see your Evidence of Coverage for more information, including the cost sharing that applies to out-of-network services. H7006 MKG BAAG ORMP-2 2024 M Confidential – Not Intended for Distribution Value. Compassion. 33
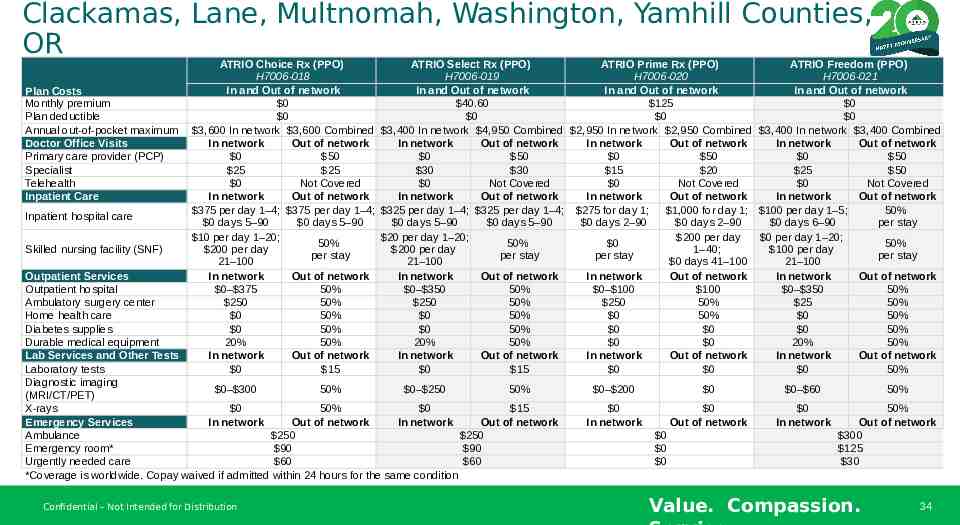
Clackamas, Lane, Multnomah, Washington, Yamhill Counties, OR 2024 PPO Medical Benefits Plan Costs Monthly premium Plan deductible Annual out-of-pocket maximum Doctor Office Visits Primary care provider (PCP) Specialist Telehealth Inpatient Care Inpatient hospital care Skilled nursing facility (SNF) ATRIO Choice Rx (PPO) ATRIO Select Rx (PPO) ATRIO Prime Rx (PPO) ATRIO Freedom (PPO) H7006-018 H7006-019 H7006-020 H7006-021 In and Out of network In and Out of network In and Out of network In and Out of network 0 40.60 125 0 0 0 0 0 3,600 In network 3,600 Combined 3,400 In network 4,950 Combined 2,950 In network 2,950 Combined 3,400 In network 3,400 Combined In network Out of network In network Out of network In network Out of network In network Out of network 0 50 0 50 0 50 0 50 25 25 30 30 15 20 25 50 0 Not Covered 0 Not Covered 0 Not Covered 0 Not Covered In network Out of network In network Out of network In network Out of network In network Out of network 375 per day 1–4; 375 per day 1–4; 325 per day 1–4; 325 per day 1–4; 275 for day 1; 1,000 for day 1; 100 per day 1–5; 50% 0 days 5–90 0 days 5–90 0 days 5–90 0 days 5–90 0 days 2–90 0 days 2–90 0 days 6–90 per stay 10 per day 1–20; 20 per day 1–20; 200 per day 0 per day 1–20; 50% 50% 0 50% 200 per day 200 per day 1–40; 100 per day per stay per stay per stay per stay 21–100 21–100 0 days 41–100 21–100 In network Out of network In network Out of network In network Out of network In network Out of network 0– 375 50% 0– 350 50% 0– 100 100 0– 350 50% 250 50% 250 50% 250 50% 25 50% 0 50% 0 50% 0 50% 0 50% 0 50% 0 50% 0 0 0 50% 20% 50% 20% 50% 0 0 20% 50% In network Out of network In network Out of network In network Out of network In network Out of network 0 15 0 15 0 0 0 50% Outpatient Services Outpatient hospital Ambulatory surgery center Home health care Diabetes supplies Durable medical equipment Lab Services and Other Tests Laboratory tests Diagnostic imaging 0– 300 50% 0– 250 50% (MRI/CT/PET) X-rays 0 50% 0 15 Emergency Services In network Out of network In network Out of network Ambulance 250 250 Emergency room* 90 90 Urgently needed care 60 60 *Coverage is worldwide. Copay waived if admitted within 24 hours for the same condition Confidential – Not Intended for Distribution 0– 200 0 0– 60 0 In network 0 Out of network 0 In network 0 0 0 50% 50% Out of network 300 125 30 Value. Compassion. 34
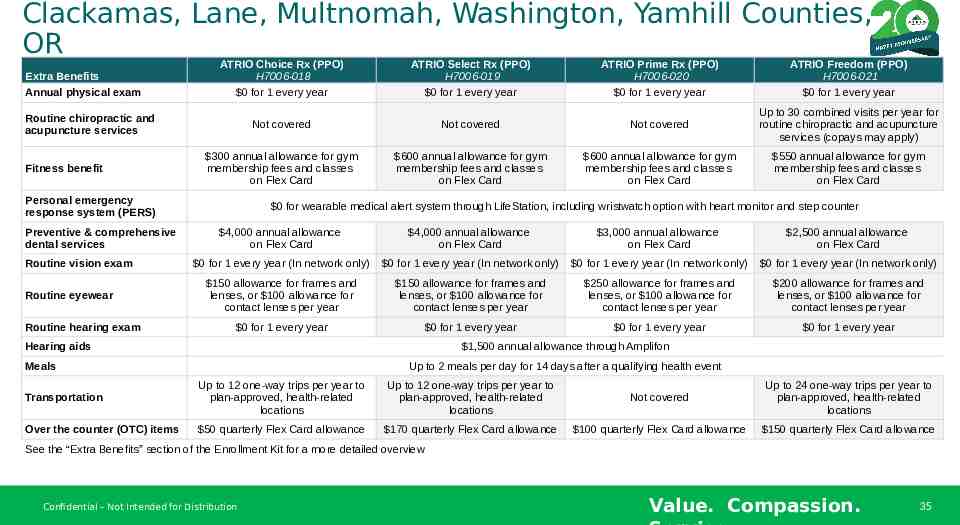
Clackamas, Lane, Multnomah, Washington, Yamhill Counties, OR 2024 PPO Extra Benefits Extra Benefits Annual physical exam ATRIO Choice Rx (PPO) H7006-018 ATRIO Select Rx (PPO) H7006-019 ATRIO Prime Rx (PPO) H7006-020 ATRIO Freedom (PPO) H7006-021 0 for 1 every year 0 for 1 every year 0 for 1 every year 0 for 1 every year Not covered Not covered Not covered Up to 30 combined visits per year for routine chiropractic and acupuncture services (copays may apply) 300 annual allowance for gym membership fees and classes on Flex Card 600 annual allowance for gym membership fees and classes on Flex Card 600 annual allowance for gym membership fees and classes on Flex Card 550 annual allowance for gym membership fees and classes on Flex Card Routine chiropractic and acupuncture services Fitness benefit Personal emergency response system (PERS) Preventive & comprehensive dental services Routine vision exam Routine eyewear Routine hearing exam 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter 4,000 annual allowance on Flex Card 4,000 annual allowance on Flex Card 3,000 annual allowance on Flex Card 2,500 annual allowance on Flex Card 0 for 1 every year (In network only) 0 for 1 every year (In network only) 0 for 1 every year (In network only) 0 for 1 every year (In network only) 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 150 allowance for frames and lenses, or 100 allowance for contact lenses per year 250 allowance for frames and lenses, or 100 allowance for contact lenses per year 200 allowance for frames and lenses, or 100 allowance for contact lenses per year 0 for 1 every year 0 for 1 every year 0 for 1 every year 0 for 1 every year Hearing aids 1,500 annual allowance through Amplifon Meals Up to 2 meals per day for 14 days after a qualifying health event Transportation Up to 12 one-way trips per year to plan-approved, health-related locations Up to 12 one-way trips per year to plan-approved, health-related locations Not covered Up to 24 one-way trips per year to plan-approved, health-related locations Over the counter (OTC) items 50 quarterly Flex Card allowance 170 quarterly Flex Card allowance 100 quarterly Flex Card allowance 150 quarterly Flex Card allowance See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Confidential – Not Intended for Distribution Value. Compassion. 35
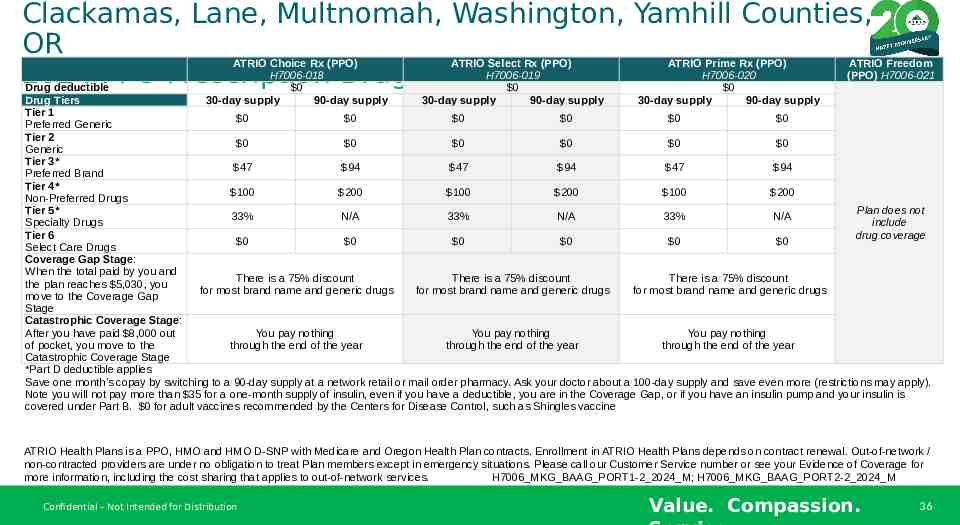
Clackamas, Lane, Multnomah, Washington, Yamhill Counties, OR 2024 PPO Prescription Drug Benefits ATRIO Choice Rx (PPO) H7006-018 0 30-day supply 90-day supply ATRIO Select Rx (PPO) H7006-019 0 30-day supply 90-day supply ATRIO Prime Rx (PPO) H7006-020 0 30-day supply 90-day supply ATRIO Freedom (PPO) H7006-021 Drug deductible Drug Tiers Tier 1 0 0 0 0 0 0 Preferred Generic Tier 2 0 0 0 0 0 0 Generic Tier 3* 47 94 47 94 47 94 Preferred Brand Tier 4* 100 200 100 200 100 200 Non-Preferred Drugs Tier 5* Plan does not 33% N/A 33% N/A 33% N/A include Specialty Drugs Tier 6 drug coverage 0 0 0 0 0 0 Select Care Drugs Coverage Gap Stage: When the total paid by you and There is a 75% discount There is a 75% discount There is a 75% discount the plan reaches 5,030, you for most brand name and generic drugs for most brand name and generic drugs for most brand name and generic drugs move to the Coverage Gap Stage Catastrophic Coverage Stage: After you have paid 8,000 out You pay nothing You pay nothing You pay nothing of pocket, you move to the through the end of the year through the end of the year through the end of the year Catastrophic Coverage Stage *Part D deductible applies Save one month’s copay by switching to a 90-day supply at a network retail or mail order pharmacy. Ask your doctor about a 100-day supply and save even more (restrictions may apply). Note you will not pay more than 35 for a one-month supply of insulin, even if you have a deductible, you are in the Coverage Gap, or if you have an insulin pump and your insulin is covered under Part B. 0 for adult vaccines recommended by the Centers for Disease Control, such as Shingles vaccine ATRIO Health Plans is a PPO, HMO and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on contract renewal. Out-of-network / non-contracted providers are under no obligation to treat Plan members except in emergency situations. Please call our Customer Service number or see your Evidence of Coverage for more information, including the cost sharing that applies to out-of-network services. H7006 MKG BAAG PORT1-2 2024 M; H7006 MKG BAAG PORT2-2 2024 M Confidential – Not Intended for Distribution Value. Compassion. 36
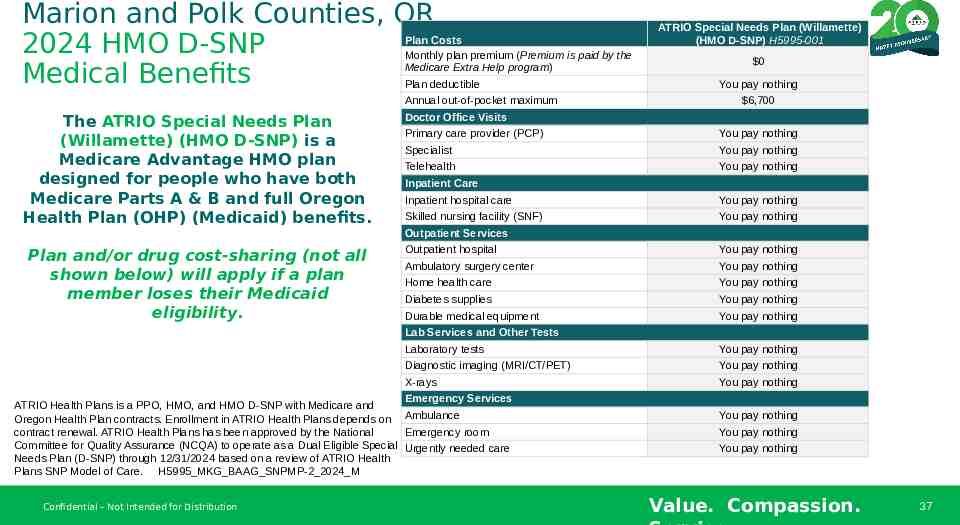
Marion and Polk Counties, OR 2024 HMO D-SNP Medical Benefits Plan Costs Monthly plan premium (Premium is paid by the Medicare Extra Help program) Plan deductible The ATRIO Special Needs Plan (Willamette) (HMO D-SNP) is a Medicare Advantage HMO plan designed for people who have both Medicare Parts A & B and full Oregon Health Plan (OHP) (Medicaid) benefits. Annual out-of-pocket maximum Doctor Office Visits ATRIO Special Needs Plan (Willamette) (HMO D-SNP) H5995-001 0 You pay nothing 6,700 Primary care provider (PCP) You pay nothing Specialist You pay nothing Telehealth You pay nothing Inpatient Care Inpatient hospital care You pay nothing Skilled nursing facility (SNF) You pay nothing Outpatient Services Plan and/or drug cost-sharing (not all shown below) will apply if a plan member loses their Medicaid eligibility. Outpatient hospital You pay nothing Ambulatory surgery center You pay nothing Home health care You pay nothing Diabetes supplies You pay nothing Durable medical equipment You pay nothing Lab Services and Other Tests Laboratory tests You pay nothing Diagnostic imaging (MRI/CT/PET) You pay nothing X-rays You pay nothing Emergency Services ATRIO Health Plans is a PPO, HMO, and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on Ambulance contract renewal. ATRIO Health Plans has been approved by the National Emergency room Committee for Quality Assurance (NCQA) to operate as a Dual Eligible Special Urgently needed care Needs Plan (D-SNP) through 12/31/2024 based on a review of ATRIO Health Plans SNP Model of Care. H5995 MKG BAAG SNPMP-2 2024 M Confidential – Not Intended for Distribution You pay nothing You pay nothing You pay nothing Value. Compassion. 37
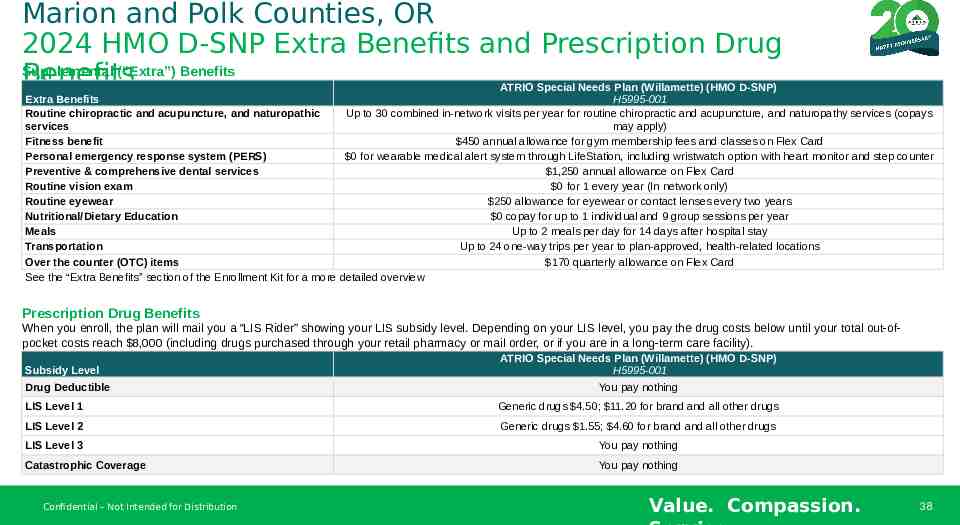
Marion and Polk Counties, OR 2024 HMO D-SNP Extra Benefits and Prescription Drug Supplemental (“Extra”) Benefits Benefits ATRIO Special Needs Plan (Willamette) (HMO D-SNP) Extra Benefits H5995-001 Routine chiropractic and acupuncture, and naturopathic Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays services may apply) Fitness benefit 450 annual allowance for gym membership fees and classes on Flex Card Personal emergency response system (PERS) 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter Preventive & comprehensive dental services 1,250 annual allowance on Flex Card Routine vision exam 0 for 1 every year (In network only) Routine eyewear 250 allowance for eyewear or contact lenses every two years Nutritional/Dietary Education 0 copay for up to 1 individual and 9 group sessions per year Meals Up to 2 meals per day for 14 days after hospital stay Transportation Up to 24 one-way trips per year to plan-approved, health-related locations Over the counter (OTC) items 170 quarterly allowance on Flex Card See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Prescription Drug Benefits When you enroll, the plan will mail you a “LIS Rider” showing your LIS subsidy level. Depending on your LIS level, you pay the drug costs below until your total out-ofpocket costs reach 8,000 (including drugs purchased through your retail pharmacy or mail order, or if you are in a long-term care facility). Subsidy Level Drug Deductible ATRIO Special Needs Plan (Willamette) (HMO D-SNP) H5995-001 You pay nothing LIS Level 1 Generic drugs 4.50; 11.20 for brand and all other drugs LIS Level 2 Generic drugs 1.55; 4.60 for brand and all other drugs LIS Level 3 You pay nothing Catastrophic Coverage You pay nothing Confidential – Not Intended for Distribution Value. Compassion. 38
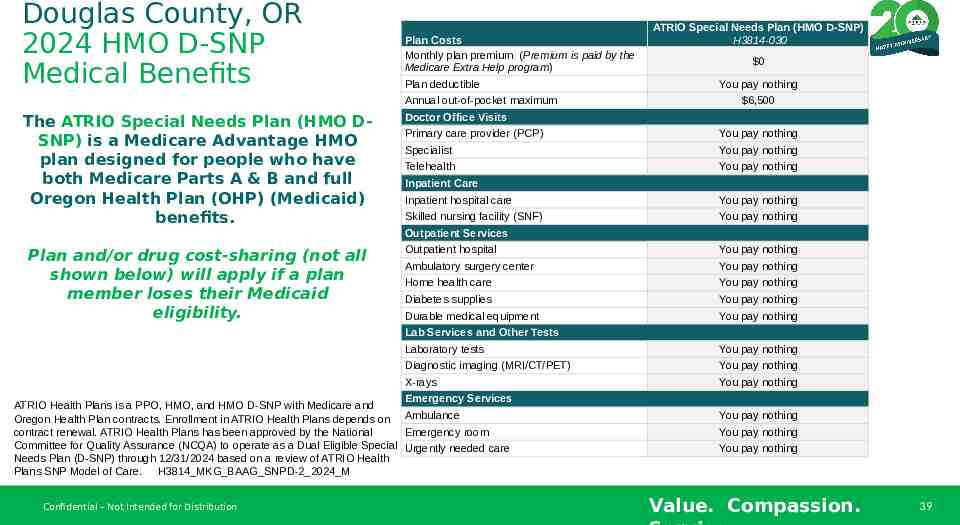
Douglas County, OR 2024 HMO D-SNP Medical Benefits The ATRIO Special Needs Plan (HMO DSNP) is a Medicare Advantage HMO plan designed for people who have both Medicare Parts A & B and full Oregon Health Plan (OHP) (Medicaid) benefits. Plan Costs Monthly plan premium (Premium is paid by the Medicare Extra Help program) Plan deductible Annual out-of-pocket maximum Doctor Office Visits ATRIO Special Needs Plan (HMO D-SNP) H3814-030 0 You pay nothing 6,500 Primary care provider (PCP) You pay nothing Specialist You pay nothing Telehealth You pay nothing Inpatient Care Inpatient hospital care You pay nothing Skilled nursing facility (SNF) You pay nothing Outpatient Services Plan and/or drug cost-sharing (not all shown below) will apply if a plan member loses their Medicaid eligibility. Outpatient hospital You pay nothing Ambulatory surgery center You pay nothing Home health care You pay nothing Diabetes supplies You pay nothing Durable medical equipment You pay nothing Lab Services and Other Tests Laboratory tests You pay nothing Diagnostic imaging (MRI/CT/PET) You pay nothing X-rays You pay nothing Emergency Services ATRIO Health Plans is a PPO, HMO, and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on Ambulance contract renewal. ATRIO Health Plans has been approved by the National Emergency room Committee for Quality Assurance (NCQA) to operate as a Dual Eligible Special Urgently needed care Needs Plan (D-SNP) through 12/31/2024 based on a review of ATRIO Health Plans SNP Model of Care. H3814 MKG BAAG SNPD-2 2024 M Confidential – Not Intended for Distribution You pay nothing You pay nothing You pay nothing Value. Compassion. 39
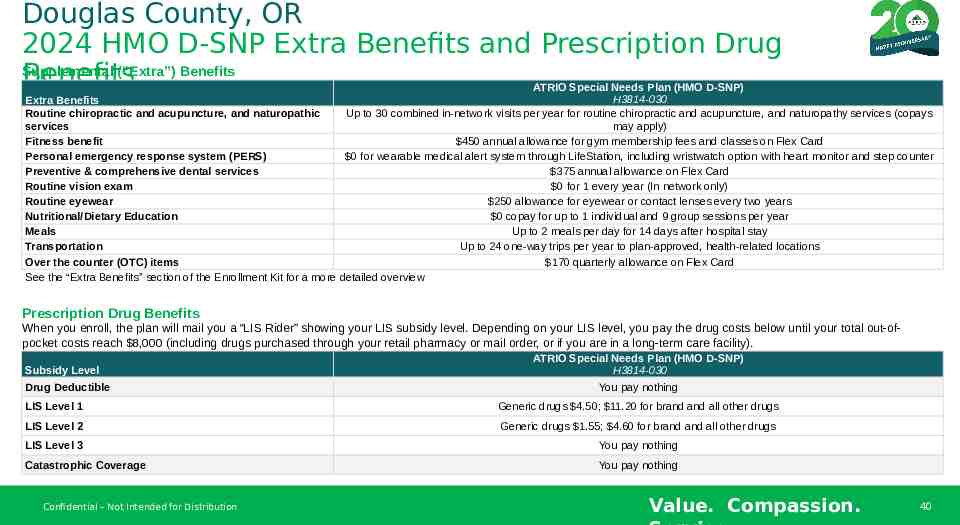
Douglas County, OR 2024 HMO D-SNP Extra Benefits and Prescription Drug Supplemental (“Extra”) Benefits Benefits ATRIO Special Needs Plan (HMO D-SNP) H3814-030 Extra Benefits Routine chiropractic and acupuncture, and naturopathic Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays services may apply) Fitness benefit 450 annual allowance for gym membership fees and classes on Flex Card Personal emergency response system (PERS) 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter Preventive & comprehensive dental services 375 annual allowance on Flex Card Routine vision exam 0 for 1 every year (In network only) Routine eyewear 250 allowance for eyewear or contact lenses every two years Nutritional/Dietary Education 0 copay for up to 1 individual and 9 group sessions per year Meals Up to 2 meals per day for 14 days after hospital stay Transportation Up to 24 one-way trips per year to plan-approved, health-related locations Over the counter (OTC) items 170 quarterly allowance on Flex Card See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Prescription Drug Benefits When you enroll, the plan will mail you a “LIS Rider” showing your LIS subsidy level. Depending on your LIS level, you pay the drug costs below until your total out-ofpocket costs reach 8,000 (including drugs purchased through your retail pharmacy or mail order, or if you are in a long-term care facility). Subsidy Level Drug Deductible ATRIO Special Needs Plan (HMO D-SNP) H3814-030 You pay nothing LIS Level 1 Generic drugs 4.50; 11.20 for brand and all other drugs LIS Level 2 Generic drugs 1.55; 4.60 for brand and all other drugs LIS Level 3 You pay nothing Catastrophic Coverage You pay nothing Confidential – Not Intended for Distribution Value. Compassion. 40
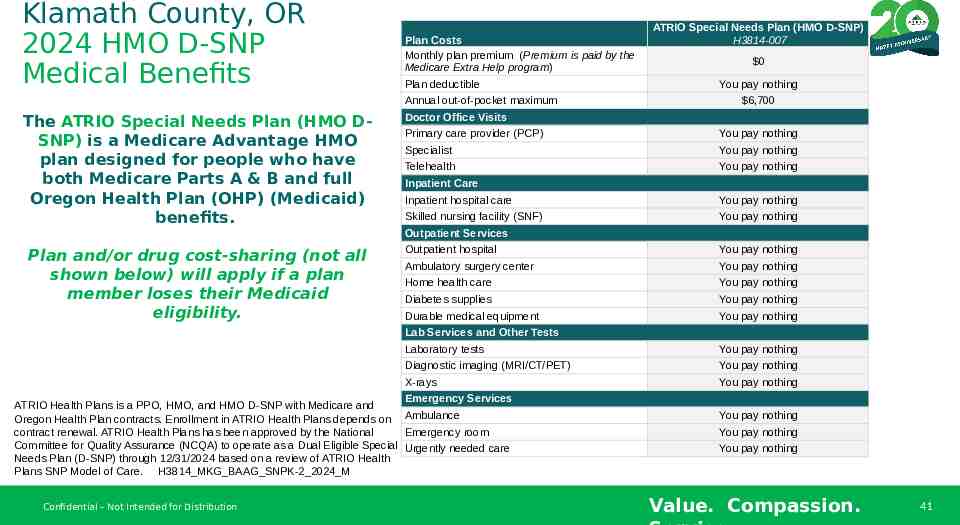
Klamath County, OR 2024 HMO D-SNP Medical Benefits The ATRIO Special Needs Plan (HMO DSNP) is a Medicare Advantage HMO plan designed for people who have both Medicare Parts A & B and full Oregon Health Plan (OHP) (Medicaid) benefits. Plan Costs Monthly plan premium (Premium is paid by the Medicare Extra Help program) Plan deductible Annual out-of-pocket maximum Doctor Office Visits ATRIO Special Needs Plan (HMO D-SNP) H3814-007 0 You pay nothing 6,700 Primary care provider (PCP) You pay nothing Specialist You pay nothing Telehealth You pay nothing Inpatient Care Inpatient hospital care You pay nothing Skilled nursing facility (SNF) You pay nothing Outpatient Services Plan and/or drug cost-sharing (not all shown below) will apply if a plan member loses their Medicaid eligibility. Outpatient hospital You pay nothing Ambulatory surgery center You pay nothing Home health care You pay nothing Diabetes supplies You pay nothing Durable medical equipment You pay nothing Lab Services and Other Tests Laboratory tests You pay nothing Diagnostic imaging (MRI/CT/PET) You pay nothing X-rays You pay nothing Emergency Services ATRIO Health Plans is a PPO, HMO, and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on Ambulance contract renewal. ATRIO Health Plans has been approved by the National Emergency room Committee for Quality Assurance (NCQA) to operate as a Dual Eligible Special Urgently needed care Needs Plan (D-SNP) through 12/31/2024 based on a review of ATRIO Health Plans SNP Model of Care. H3814 MKG BAAG SNPK-2 2024 M Confidential – Not Intended for Distribution You pay nothing You pay nothing You pay nothing Value. Compassion. 41
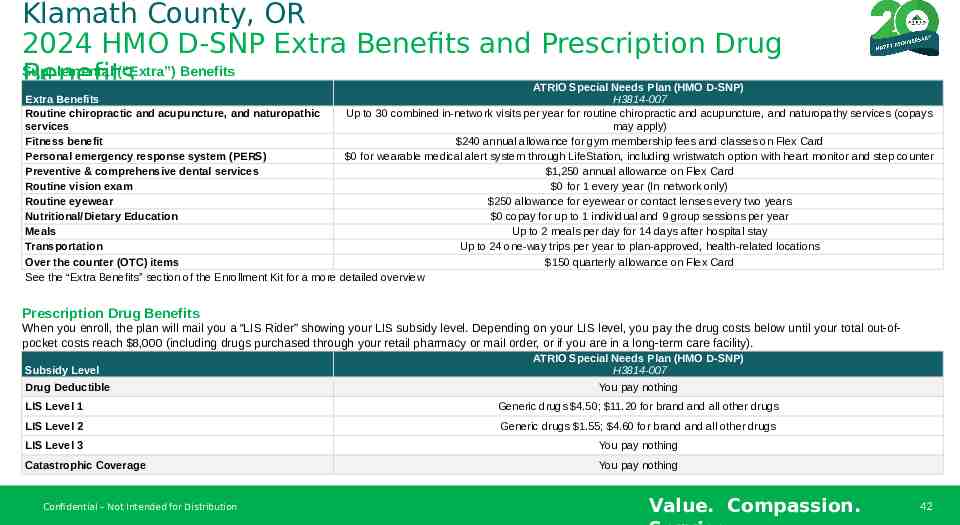
Klamath County, OR 2024 HMO D-SNP Extra Benefits and Prescription Drug Supplemental (“Extra”) Benefits Benefits ATRIO Special Needs Plan (HMO D-SNP) Extra Benefits H3814-007 Routine chiropractic and acupuncture, and naturopathic Up to 30 combined in-network visits per year for routine chiropractic and acupuncture, and naturopathy services (copays services may apply) Fitness benefit 240 annual allowance for gym membership fees and classes on Flex Card Personal emergency response system (PERS) 0 for wearable medical alert system through LifeStation, including wristwatch option with heart monitor and step counter Preventive & comprehensive dental services 1,250 annual allowance on Flex Card Routine vision exam 0 for 1 every year (In network only) Routine eyewear 250 allowance for eyewear or contact lenses every two years Nutritional/Dietary Education 0 copay for up to 1 individual and 9 group sessions per year Meals Up to 2 meals per day for 14 days after hospital stay Transportation Up to 24 one-way trips per year to plan-approved, health-related locations Over the counter (OTC) items 150 quarterly allowance on Flex Card See the “Extra Benefits” section of the Enrollment Kit for a more detailed overview Prescription Drug Benefits When you enroll, the plan will mail you a “LIS Rider” showing your LIS subsidy level. Depending on your LIS level, you pay the drug costs below until your total out-ofpocket costs reach 8,000 (including drugs purchased through your retail pharmacy or mail order, or if you are in a long-term care facility). Subsidy Level Drug Deductible ATRIO Special Needs Plan (HMO D-SNP) H3814-007 You pay nothing LIS Level 1 Generic drugs 4.50; 11.20 for brand and all other drugs LIS Level 2 Generic drugs 1.55; 4.60 for brand and all other drugs LIS Level 3 You pay nothing Catastrophic Coverage You pay nothing Confidential – Not Intended for Distribution Value. Compassion. 42
Star Ratings How are Star Ratings determined? The two main types of Star Ratings are: 1. An Overall Star Rating that combines all of our plan's scores 2. Summary Star Ratings that focus on our medical (Part C) and our prescription drug services (Part D) Some of the areas Medicare reviews for these ratings include: How our members rate our plan's services and care How well our doctors detect illnesses and keep members healthy How well our plan helps our members use recommended and safe prescription medications. Confidential – Not Intended for Distribution Value. Compassion.
Need Help? I am here for you. Look up doctors, hospitals, specialists and clinics to make sure they’re part of ATRIO Health Plans provider network Check your prescription medications to make sure they're included in the drug list and anticipated costs Understand how a Medicare Advantage plan from ATRIO Health Plans can work with the care you receive from the VA or TRICARE For Life coverage Find out if you’re eligible for more benefits such as Extra Help Access additional services, including benefits available to ATRIO Health Plan members Confidential – Not Intended for Distribution Value. Compassion.
Ready to Enroll? We are here to assist you! Agent Name INSERT PHOTO Licensed Sales Agent Agent Phone # Agent Email ATRIO Health Plans is a PPO, HMO, and HMO D-SNP with Medicare and Oregon Health Plan contracts. Enrollment in ATRIO Health Plans depends on contract renewal. Confidential – Not Intended for Distribution Value. Compassion.