The Brighton Experience
















34 Slides1.73 MB
The Brighton Experience
ARK feasibility Started April 18th Finishes July 18th Highlight key aspects of preparation and implementation Share audit and feedback data
Phase 1: Preparation 1. Familiarise self with ARK and identify useful implementation materials in resources Access the online tool Review the resources Sign up to the champions forum
Phase 1: Preparation 2. List local procedures and how ARK would fit into existing structures Outline the flow of acute general medical inpatients in your hospital Consider what Felt we had a good understanding – didn’t map robustly Underestimated the number processes already existof ED clerkings Microguide and pharmacy pages. Didn’t consider wording of duration recommendations. Could be less didactic? Identify the main barriers / strategies that could be used to overcome these barriers .
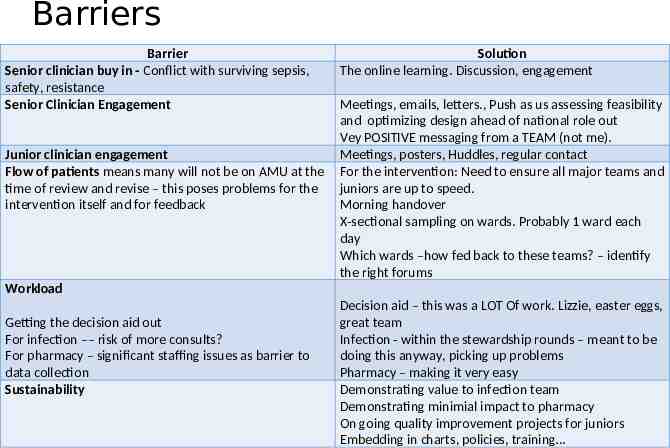
Barriers Barrier Senior clinician buy in - Conflict with surviving sepsis, safety, resistance Senior Clinician Engagement Junior clinician engagement Flow of patients means many will not be on AMU at the time of review and revise – this poses problems for the intervention itself and for feedback Solution The online learning. Discussion, engagement Meetings, emails, letters., Push as us assessing feasibility and optimizing design ahead of national role out Vey POSITIVE messaging from a TEAM (not me). Meetings, posters, Huddles, regular contact For the intervention: Need to ensure all major teams and juniors are up to speed. Morning handover X-sectional sampling on wards. Probably 1 ward each day Which wards –how fed back to these teams? – identify the right forums Workload Getting the decision aid out For infection –– risk of more consults? For pharmacy – significant staffing issues as barrier to data collection Sustainability Decision aid – this was a LOT Of work. Lizzie, easter eggs, great team Infection - within the stewardship rounds – meant to be doing this anyway, picking up problems Pharmacy – making it very easy Demonstrating value to infection team Demonstrating minimial impact to pharmacy On going quality improvement projects for juniors Embedding in charts, policies, training
Phase 1: Preparation 2. List local procedures and how ARK would fit into existing structures Think about how prescribers will record the ARK antibiotic prescription categorisation Stickers on the drug chart New Chart in preparation Key piece of work for the ARK Core team, multiple drafts, piloting Review your trust’s ‘review and revise’ audit data. ‘Patient safety thermometer’ Very variable stop rates – 3-22% On close scrutiny, not credible
Phase 1: Preparation 3. Obtain board level support List what board level support should be sought Medical Director? Director of Quality Improvement . Director of Medical Education. Chief Nurse. Investigate whether the ARK online tool could be incorporated into your Trust’s learning and development programme, Presented to Med Education Director / committee – slots on F1, F2, CMT teaching DIPC, Infection Control Lead - to incorporate into mandatory training Ask your Trust’s responsible officer how to get the ARK online tool included in the appraisal process. Medical Director .
Phase 1: Preparation 4. Identify Members of the ARK core team Microbiologist AMU / ID consultant antibiotic pharmacists AMU charge nurse AMU pharmacist infection trainees / ACFs AMU Junior
Phase 2: Implementation Planning (t-4 months) 1. Familiarise ARK Core Team with ARK 2. Hold an Initial Planning Meeting (March 8th) Plan kick-off meetings Discuss how you will gather data to assess the adoption and impact of the intervention Discuss how to feedback information about audit data Discuss how to make ARK sustainable in the long term
Programme of Kick Off Meetings Grand Round (March 22) Team meetings AMU (Resp) Elderly Endocrine Gastro HIV ICU Haem/Onc (Emergency med) Healthcare professional meetings F1s F2s CMTs SpRs Pharmacists Nurses Med Ed Dept Infection Control Dept
Phase 2: Implementation Planning: 1. Familiarise ARK Core Team with ARK 2. Hold an Initial Planning Meeting 1.Plan kick-off meetings 2.Discuss how you will gather data to assess the adoption and impact of the intervention Point prevalence tool and programme of assessments 3.Discuss how to feedback information about audit data Identifying points of feedback e.g. AMU handover, team governance and teaching meetings 4.Discuss how to make ARK sustainable in the long term Embedded – decision aid, induction, mandatory training Audit and feedback .
Phase 2: Implementation Planning 3. Pilot local tools / processes Data collection tool Decision aid 4. Get Necessary Approvals Integrate the Decision Aid into the existing prescription system Drugs and therapeutics committee Antimicrobial stewardship lead Get approval for use of the Patient Leaflet Drugs and therapeutics committee Obtain learning and development office approval for ARK online tool Done in phase 1
Phase 3: Organise Kick-Off (t-2 months) 1. Identify key members of the wider clinical team - Finalise a list of essential people 2. Organise and publicise kick off meetings 3. Get staff to complete the online tool before attending the kick-off meeting.
Essential People All AMU Consultants 1-2 named consultants from each medical team (elderly, resp, gasto, Endo) All the ID/micro team The lead medical SpR AMU matrons AMU pharmacists Senior Infection Control NursesC Chair of DTC Director of Med Ed
Phase 3: Organise Kick-Off (t-2 months) 1. Identify key members of the wider clinical team - Finalise a list of essential people 2. Organise and publicise kick off meetings Emails from the Medical Director to all medical staff One side summaries – doctors and nurses 3. Get staff to complete the online tool before attending the kick-off meeting. Hard but REALLY useful
Phase 4: Get ready for Implementation (t-2 weeks) Remind staff to complete the online tool before kick off Email reminders Run kickoff meetings Grand round and clinical team slide sets Arrange regular discussions with clinical teams In pre existing sessions
Phase 5: Implementation starts April 18th - Tuesday after Easter end of school holidays. 4 days before ECCMID. Never an ideal time. Presence on AMU Face to face reminders in AMU Visibility “The reason this has worked is that you didn’t just introduce it and then comeback 3 months later and say it hasn’t really worked. You were visible regularly in AMU, keeping up the profile, feeding back and discussing.”
Phase 6: On going implementation 1) Collect objective evidence 2) Facilitate regular discussions 3) Facilitate ongoing implementation 4) Complete implementation checklist
ARK feasibility Started April 18th (Tuesday after Easter end of school holidays. 4 days before ECCMID.) Finishes July 18th Highlight key aspects of preparation and implementation Share audit and feedback data
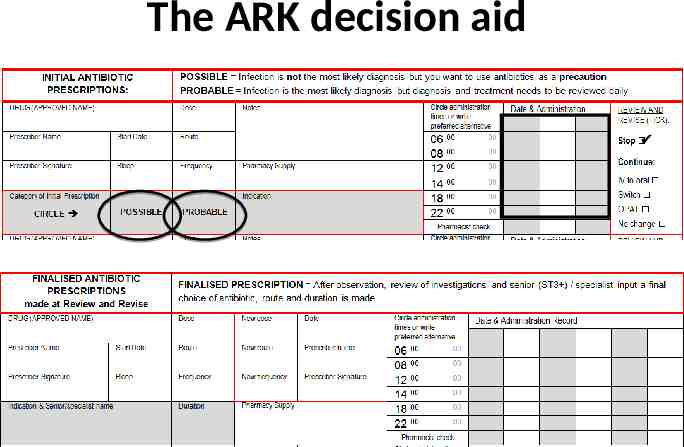
The ARK decision aid
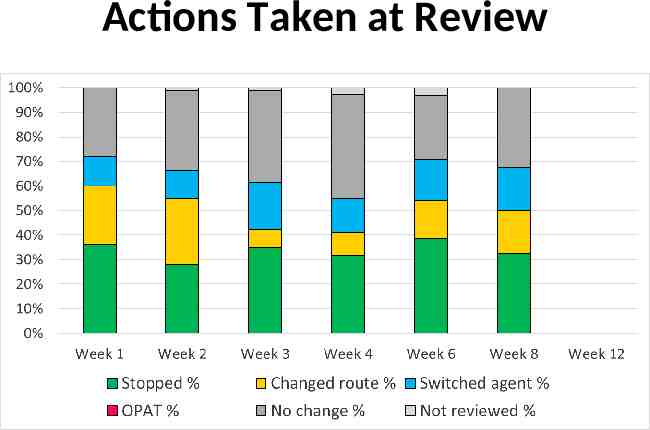
ARK audit data Point prevalence surveys Weeks 1, 2, 3, 4, 6 and 8 (week 12 this week) Using ARK-Hospital data collection tool Variety of medical specialties: – Acute medicine, respiratory, elderly care, endocrine, gastroenterology Purpose feedback to clinical teams
ARK audit data weeks 1-8 502 prescriptions
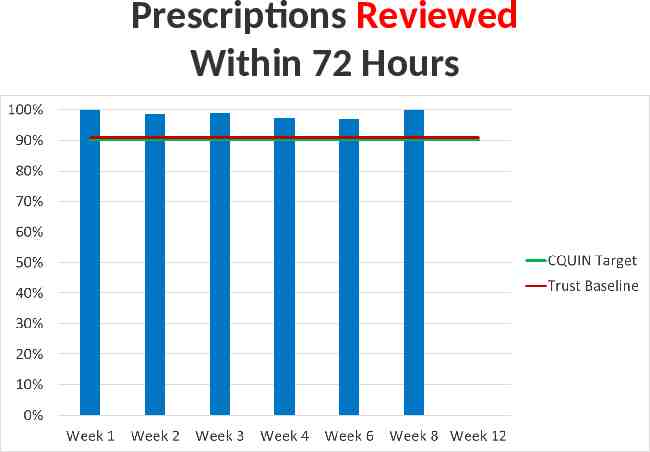
Prescriptions Reviewed Within 72 Hours
Prescriptions Categorised using ARK Decision Aid at Initial Prescription New target
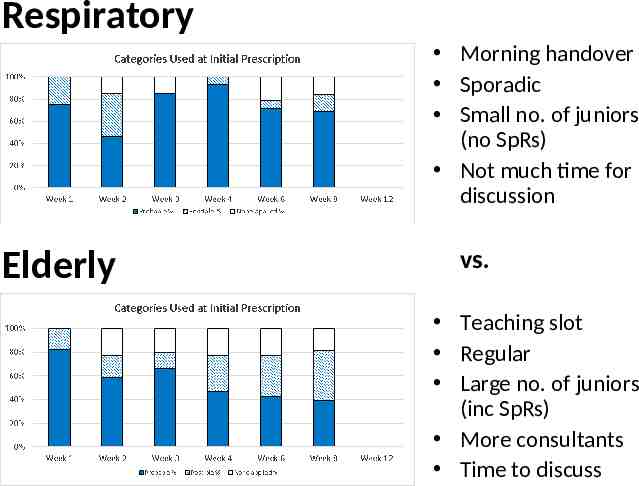
Categories Used at Initial Prescription
Prescriptions Stopped Within 72 Hour Review
Actions Taken at Review
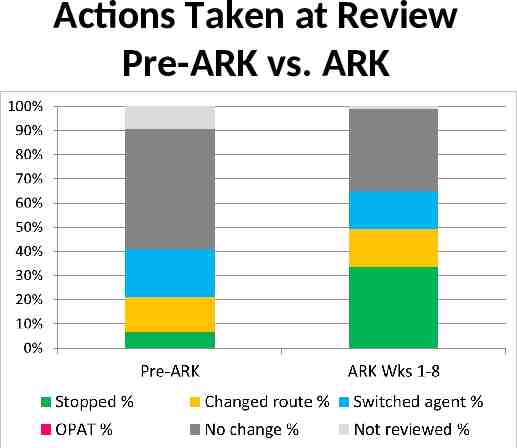
Actions Taken at Review Pre-ARK vs. ARK
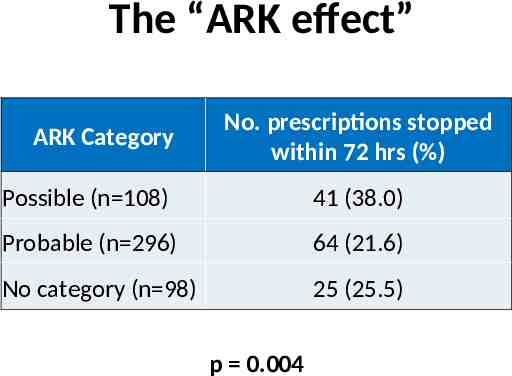
The “ARK effect” ARK Category No. prescriptions stopped within 72 hrs (%) Possible (n 108) 41 (38.0) Probable (n 296) 64 (21.6) No category (n 98) 25 (25.5) p 0.004
Feedback to clinical teams Specialty Meeting Acute medicine Bed meeting Audience Juniors doctors, consultants, nurses, pharmacists, bed managers, ward clerks Departmental teaching Junior doctors, consultants Respiratory Morning handover Juniors doctors, consultants, nurses, pharmacists, OTs, PTs Endocrine M&M meeting ( ward huddles) Junior doctors, consultants, nurse in charge Elderly
Feedback to clinical teams Quick & succinct 5 mins in total: 2 mins 2 mins 1 min
Respiratory Morning handover Sporadic Small no. of juniors (no SpRs) Not much time for discussion Elderly vs. Teaching slot Regular Large no. of juniors (inc SpRs) More consultants Time to discuss
Respiratory Morning handover Sporadic Small no. of juniors (no SpRs) Not much time for discussion Elderly vs. Teaching slot Regular Large no. of juniors (inc SpRs) More consultants Time to discuss
Helpful resources Guidance on 72hr r/v decisions Collection of clinical vignettes Posters for doctors and nurses






