Social Work and Care Coordination – Successful Models: Home



28 Slides1.37 MB
Social Work and Care Coordination – Successful Models: Home and Community Services Network W. June Simmons, MSW - CEO Partners in Care Foundation September 19, 2012 CalSWEC Aging Summit 1
Agenda An historic opportunity for positive change Addressing social, environmental and self-care components that drive health outcomes Unique characteristics required in changing environment – a new business model – Strategies for LTSS impacting Medicare and MediCal service use/health outcomes – Home & Community Services Network 2
Moving from Presenting Problem to Presenting Person Managed care seeks best care for best cost, so represents an opportunity for major change The Duals demonstration moves the risk for nursing home to health plans and provider groups LTSS resources are crucial to success – reduces both nursing home and Medicare costs “Buy vs. build” and other competing forces
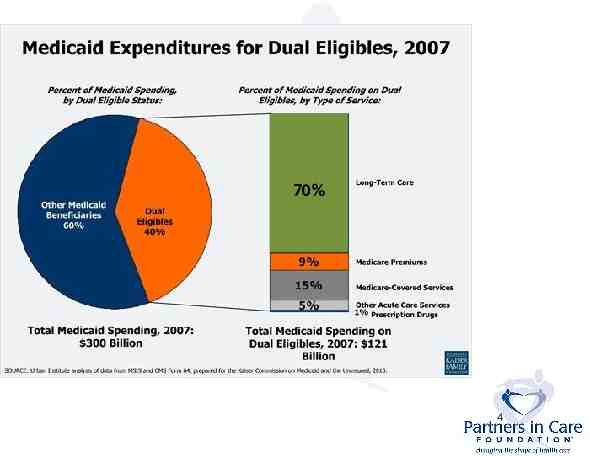
70% 4
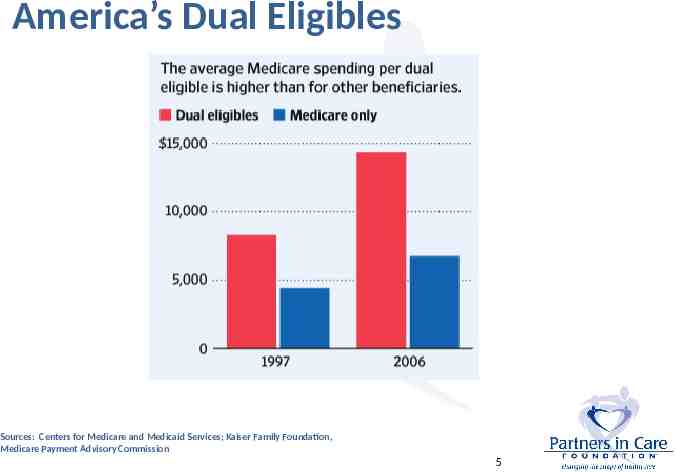
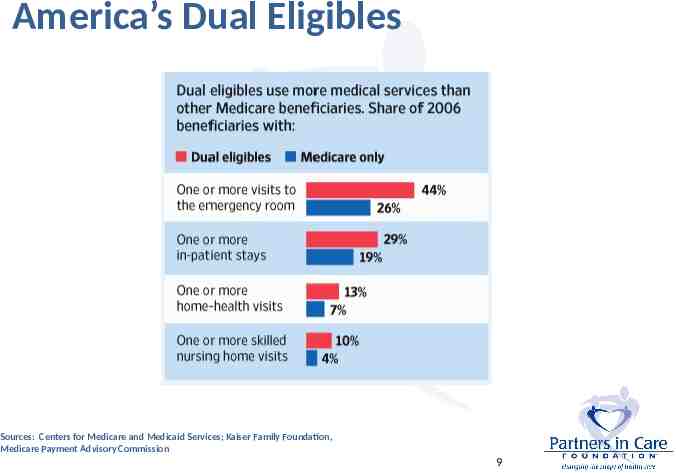
America’s Dual Eligibles Sources: Centers for Medicare and Medicaid Services; Kaiser Family Foundation, Medicare Payment Advisory Commission 5
Duals Demonstration Project – How the Risk Will Shift Total financial responsibility for the full continuum of Medicare and Medi-Cal services will now include: medical care behavioral health services, and long-term services and supports (LTSS): – – – – In-Home Supportive Services (IHSS) Community-Based Adult Services (CBAS) Multipurpose Senior Services Program (MSSP) Nursing facilities when needed Social/environmental/self-care supports help dual eligible beneficiaries maintain health and extend living at home - this can reduce costs 6
Why the Costs are so High Nursing Home is expensive and feared For Medicare, Duals’ high costs driven by elevated need for acute care due to increased prevalence of chronic disease associated with age, disability, poverty AND gaps in the system Medical interventions alone are not enoughneed proven strategies for LTSS in home and self-care - need targeted evidence-based approaches 8
America’s Dual Eligibles Sources: Centers for Medicare and Medicaid Services; Kaiser Family Foundation, Medicare Payment Advisory Commission 9
Clustered “products” enhance results MSSP model: assessment and mobilizing social and environmental resources Stabilizes at home and alternate kinds of help Coordination with CBAS, IHSS and mental health in place Now must couple with other new approaches: – Transitions – post-hospital interventions – Home-Meds and In-Home Palliative Care – Evidence-based self-management programs
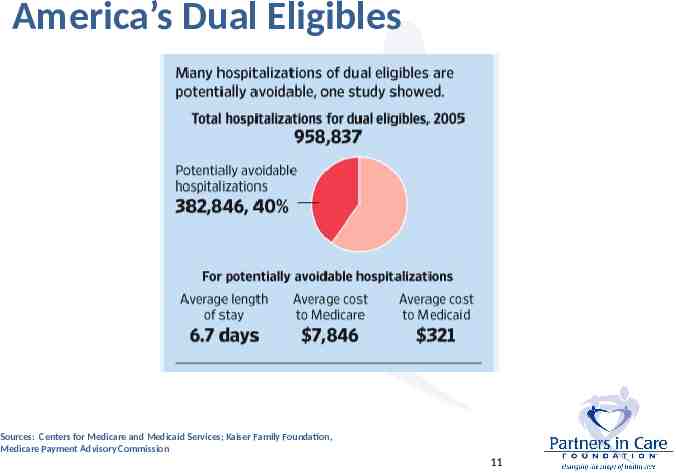
America’s Dual Eligibles Sources: Centers for Medicare and Medicaid Services; Kaiser Family Foundation, Medicare Payment Advisory Commission 11
How Home and Community Services Address and Improve Health Outcomes – thus cost effective for both Medi-Cal and Medicare Multiple, complex chronic conditions & self-care Evidence-based enhanced self-care programs (e.g, Chronic Disease Self Management (CDSMP), Diabetes Self Management (DSMP) Complex medications/adherence (HomeMeds ) Multiple ER visits – gaps in care/communication Post-hospital support to avoid readmissions Nursing home diversion/return to community In-home palliative care in last year of life 12
How to Best Care for the Duals to Achieve Optimal Health Outcomes 13
Hot Spotting - Targeting High costs come from specific target groups, where the investment of a new intervention yields better health and quality of life outcomes while driving down costs Evidence-based self-management maintains health Identify complex patients – screen consistently Medi-Cal targets keeping people out of nursing homes and we can also Impact Medicare more directly by reducing ER, hospital admissions and readmissions
What is Long Term Care? Encompasses a wide array of medicine, social, personal and supportive and specialized housing services Social and environmental factors are crucial to determining full positive impact of medicine Needed by people who have lost some capacity for self-care Care at home or in a nursing home Most who need LTC are over age 76 (63%) 15
Activities of Daily Living (ADLs) Personal care activities people engage in every day Fundamental to caring for oneself to maintain personal independence Assessment determines level of care/ assistance needed Certifies LTC level of care/payment level 16
ADL Functions ADL Functions – – – – – – – – Bathing Dressing Grooming Mouth care Toileting Transferring bed/chair Climbing stairs Eating Each function is rated to determine level of support required: -INDEPENDENT -NEEDS SOME HELP -VERY DEPENDENT -CANNOT DO 17
Instrumental Activities of Daily Living (IADLs) Related to independent living Valuable for evaluating level of disease Determinant of person’s ability to care for themselves and their environment 18
IADL Functions IADL Functions – – – – – – – – Shopping Cooking Managing medications Using the phone and looking up phone numbers Doing housework Doing laundry Driving or using public transportation Managing finances Each function is rated to determine level of support required: -INDEPENDENT -NEEDS SOME HELP -VERY DEPENDENT -CANNOT DO 19
Home and Community LTC System Helps Avoid Nursing Home Placement Care at home can sustain independence Comprehensive in-home assessment identifies risks, basis to craft an in-home careplan Currently 6 separate MSSP agencies across LA County and 41 in the state offer MSSP care in the home to Medi-Cal beneficiaries MSSP program moves under managed care and is a great prototype for care coordination Work across agency lines to integrate
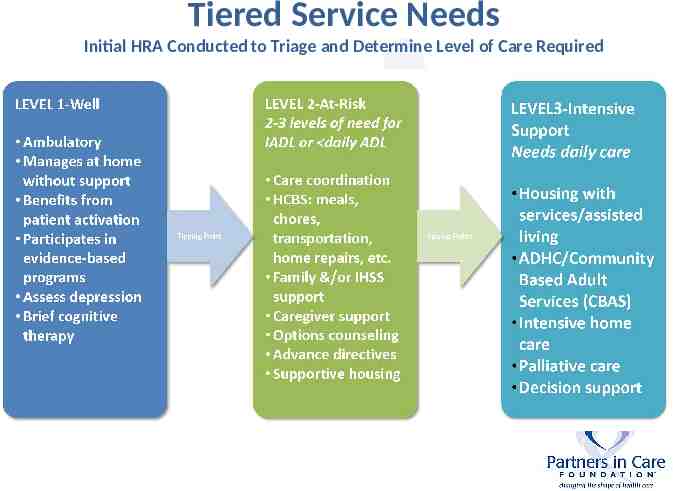
Tiered Service Needs Initial HRA Conducted to Triage and Determine Level of Care Required
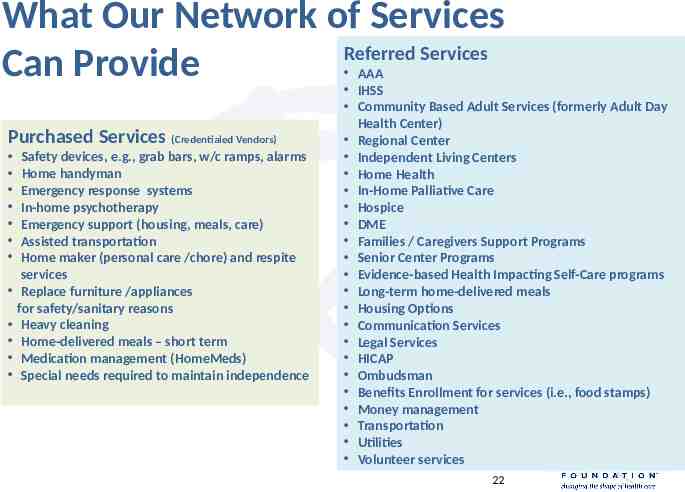
What Our Network of Services Referred Services Can Provide Purchased Services (Credentialed Vendors) Safety devices, e.g., grab bars, w/c ramps, alarms Home handyman Emergency response systems In-home psychotherapy Emergency support (housing, meals, care) Assisted transportation Home maker (personal care /chore) and respite services Replace furniture /appliances for safety/sanitary reasons Heavy cleaning Home-delivered meals – short term Medication management (HomeMeds) Special needs required to maintain independence AAA IHSS Community Based Adult Services (formerly Adult Day Health Center) Regional Center Independent Living Centers Home Health In-Home Palliative Care Hospice DME Families / Caregivers Support Programs Senior Center Programs Evidence-based Health Impacting Self-Care programs Long-term home-delivered meals Housing Options Communication Services Legal Services HICAP Ombudsman Benefits Enrollment for services (i.e., food stamps) Money management Transportation Utilities Volunteer services 22
AAAs and Sponsors of MSSP Offer Access and Strengths Area Agencies on Aging – crucial access point MSSP sponsors can evolve “prototype” into expanded tiered home care approaches Scaling up from solid base and clinical infrastructure safer than “reinventing” “Community” is a specialty practice expertise Evidence-based self-care will be next generation of added interventions - phased
How We Work Together Home and Community Services Network – Broad geographic coverage with in-home Care Coordination through a central portal – Common assessment tool and EMR – Multi-lingual/cultural competence/home experts – Contracted, credentialed network of trusted vendors and linked partnerships – Administrative simplicity with full access to both arrange and purchase community care resources 24
Home and Community Services Network - Key Elements Full geographic coverage of L.A. County - one portal for all Credentialed contractors for purchase of home and community-based services and personal care Common data system Strong business case MSSP model is prototype – Build on base of 3,400 clients/170 care coordination staff – RNs and Social Workers in 7 locations – Cost effective, proven, and uniform model of care Ability to scale up and differentiate – Tiered care management models possible 25
Current System Area Agencies on Aging/ senior centers and core services Caregiver Resources Centers In-home Supportive Services (IHSS) Adult day health/Community-Based Adult Services (CBAS) MSSP – nursing home diversion Mental Health Services
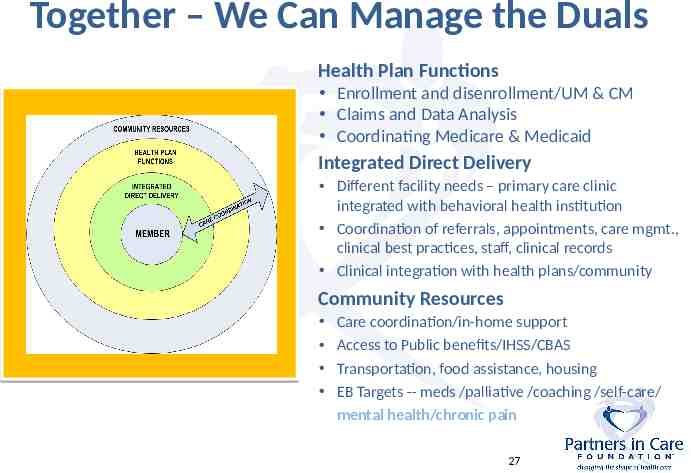
Together – We Can Manage the Duals Health Plan Functions Enrollment and disenrollment/UM & CM Claims and Data Analysis Coordinating Medicare & Medicaid Integrated Direct Delivery Different facility needs – primary care clinic integrated with behavioral health institution Coordination of referrals, appointments, care mgmt., clinical best practices, staff, clinical records Clinical integration with health plans/community Community Resources Care coordination/in-home support Access to Public benefits/IHSS/CBAS Transportation, food assistance, housing EB Targets -- meds /palliative /coaching /self-care/ mental health/chronic pain 27
The Time is Now For more information contact: -June Simmons, Partners in Care Foundation [email protected] (818) 837-3775 -