SERVICE COORDINATION OVERVIEW CHC PHASE 3 PROVIDER SUMMIT


42 Slides679.09 KB
SERVICE COORDINATION OVERVIEW CHC PHASE 3 PROVIDER SUMMIT KEVIN HANCOCK JEANNE PARISI OFFICE OF LONG-TERM LIVING DEPARTMENT OF HUMAN SERVICES June 2018
AGENDA 1. Objectives of Service Coordination in Community HealthChoices (CHC) 2. Current Service Coordination Requirements in Fee-for-Service (FFS) Waivers vs. CHC Service Coordination Requirements 3. Continuity of Care for CHC Implementation 4. Service Coordination as an Administrative Function of CHC 5. Service Coordinator and Service Coordination Supervisor Requirements in CHC 6. Comprehensive Needs Assessments and Reassessments 7. Person-Centered Service Planning (PCSP) 8. Care Plan vs. LTSS Plan 9. The Role of the Person-Centered Planning Team (PCPT) 10.Coordination with the Non-Medicaid Community-Based Services 11.Lessons Learned from the Southwest Implementation 12.Questions 2
OBJECTIVES OF SERVICE COORDINATION IN CHC The primary objective of service coordination is to oversee the person-centered service planning process and to provide support for CHC program participants, specifically those individuals in need of long-term supports and services (LTSS) and those with unmet needs, in the following ways: 1. The identification of needed services through the Comprehensive Needs Assessment process. 2. The assurance of appropriate service delivery that supports both a participant’s needs and their preferences through the management of the person-centered planning process and the development and implementation of the participant’s person-centered service plan. 3. The coordination of the participant’s long-term care services with all of their other services including those provided by Medicare, behavioral health, and Medicaid physical health. 3
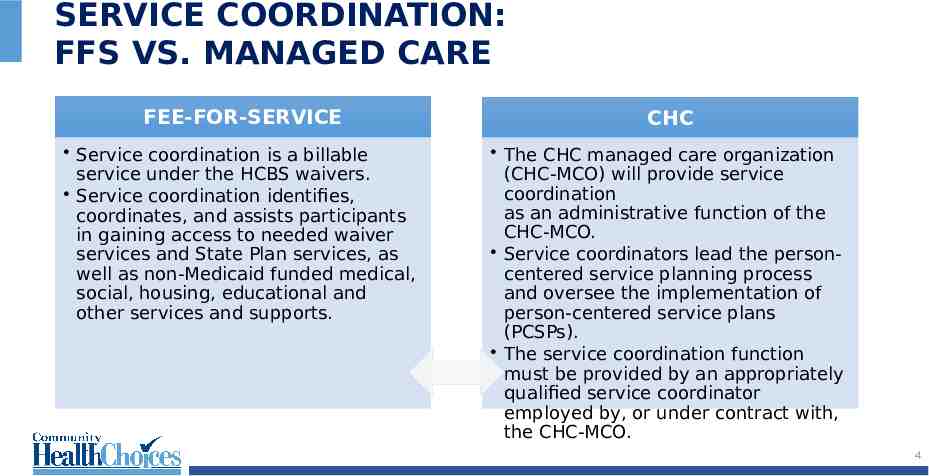
SERVICE COORDINATION: FFS VS. MANAGED CARE FEE-FOR-SERVICE CHC Service coordination is a billable service under the HCBS waivers. Service coordination identifies, coordinates, and assists participants in gaining access to needed waiver services and State Plan services, as well as non-Medicaid funded medical, social, housing, educational and other services and supports. The CHC managed care organization (CHC-MCO) will provide service coordination as an administrative function of the CHC-MCO. Service coordinators lead the personcentered service planning process and oversee the implementation of person-centered service plans (PCSPs). The service coordination function must be provided by an appropriately qualified service coordinator employed by, or under contract with, the CHC-MCO. 4
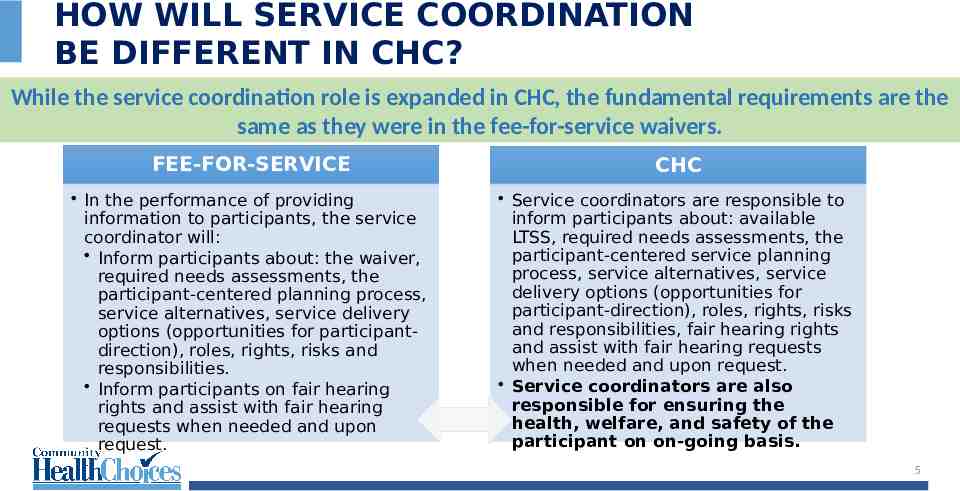
HOW WILL SERVICE COORDINATION BE DIFFERENT IN CHC? While the service coordination role is expanded in CHC, the fundamental requirements are the same as they were in the fee-for-service waivers. FEE-FOR-SERVICE CHC In the performance of providing information to participants, the service coordinator will: Inform participants about: the waiver, required needs assessments, the participant-centered planning process, service alternatives, service delivery options (opportunities for participantdirection), roles, rights, risks and responsibilities. Inform participants on fair hearing rights and assist with fair hearing requests when needed and upon request. Service coordinators are responsible to inform participants about: available LTSS, required needs assessments, the participant-centered service planning process, service alternatives, service delivery options (opportunities for participant-direction), roles, rights, risks and responsibilities, fair hearing rights and assist with fair hearing requests when needed and upon request. Service coordinators are also responsible for ensuring the health, welfare, and safety of the participant on on-going basis. 5
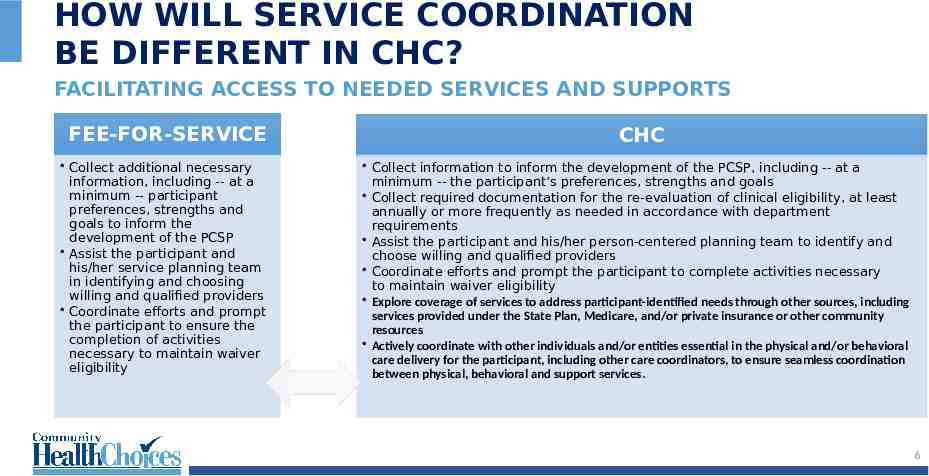
HOW WILL SERVICE COORDINATION BE DIFFERENT IN CHC? FACILITATING ACCESS TO NEEDED SERVICES AND SUPPORTS FEE-FOR-SERVICE Collect additional necessary information, including -- at a minimum -- participant preferences, strengths and goals to inform the development of the PCSP Assist the participant and his/her service planning team in identifying and choosing willing and qualified providers Coordinate efforts and prompt the participant to ensure the completion of activities necessary to maintain waiver eligibility CHC Collect information to inform the development of the PCSP, including -- at a minimum -- the participant’s preferences, strengths and goals Collect required documentation for the re-evaluation of clinical eligibility, at least annually or more frequently as needed in accordance with department requirements Assist the participant and his/her person-centered planning team to identify and choose willing and qualified providers Coordinate efforts and prompt the participant to complete activities necessary to maintain waiver eligibility Explore coverage of services to address participant-identified needs through other sources, including services provided under the State Plan, Medicare, and/or private insurance or other community resources Actively coordinate with other individuals and/or entities essential in the physical and/or behavioral care delivery for the participant, including other care coordinators, to ensure seamless coordination between physical, behavioral and support services. 6
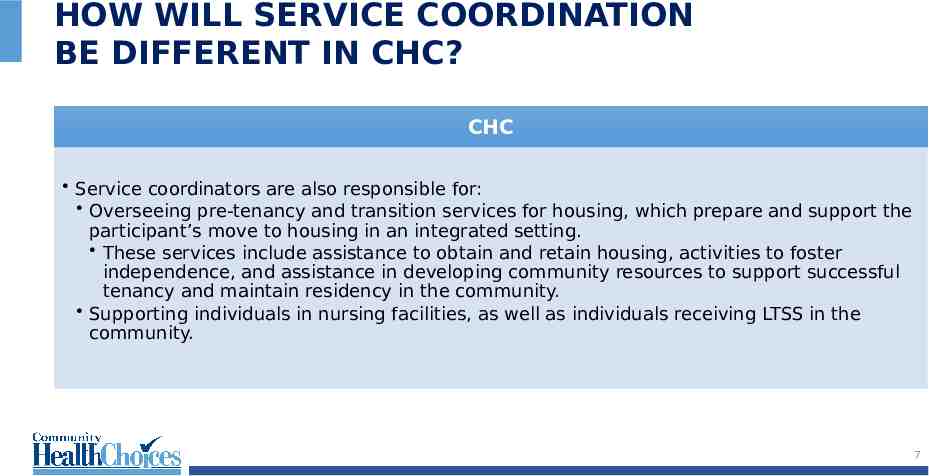
HOW WILL SERVICE COORDINATION BE DIFFERENT IN CHC? CHC Service coordinators are also responsible for: Overseeing pre-tenancy and transition services for housing, which prepare and support the participant’s move to housing in an integrated setting. These services include assistance to obtain and retain housing, activities to foster independence, and assistance in developing community resources to support successful tenancy and maintain residency in the community. Supporting individuals in nursing facilities, as well as individuals receiving LTSS in the community. 7
CONTINUITY OF CARE MCOs are required to contract with all willing and qualified existing LTSS Medicaid providers for 180 days after CHC implementation. The 180 day continuity of care requirement includes service coordination entities. Participants may keep their existing LTSS providers for the 180-day continuity of care period after CHC implementation. Participants may keep their existing physical health providers for the 60-day continuity of care period after CHC implementation. For nursing facility residents, participants will be able to stay in their nursing facility as long as they need this level of care, unless they choose to move. The commonwealth will conduct ongoing monitoring to ensure the MCOs maintain provider networks that enable participants choice of provider for needed services. For all participants, the CHC-MCO must comply with continuity of care requirements for continuation of providers, services, and any ongoing course of treatment outlined in MA Bulletin 99-03-13, Continuity of Care for Recipients Transferring Between and Among Fee-for-Service and Managed Care Organizations. 8
SERVICE COORDINATION AS AN ADMINISTRATIVE FUNCTION The CHC-MCO must provide service coordination as an administrative function through appropriately qualified staff or contracts with service coordination entities. Service coordinators will either be directly employed by the CHC-MCOs or will support this service through a subcontractor relationship after the continuity-ofcare period expires. Currently, service coordinators serve as fee-for-service providers in the HCBS waivers. 9
PROPOSED SERVICE COORDINATOR STAFFING REQUIREMENTS (DRAFT) Service Coordinators must have a Bachelor’s degree in social work, psychology, or other related fields with practicum experience, or in lieu of a Bachelor’s degree have at least three (3) or more years’ experience in a social service or healthcare related setting. Service Coordinators hired prior to the CHC zone implementation date must have the qualifications and standards proposed by the CHC-MCOs and approved by the Department. Service Coordinator Supervisors must have a Master’s degree and three (3) years of relevant experience with a commitment to obtain either a Pennsylvania social work or mental health professional license within one year of hire. Service Coordinator supervisors hired prior to the CHC zone implementation date (who do not have a license) must either: 1) obtain a license within the first year of this Agreement, or 2) have the qualifications and standards proposed by the CHCMCOs and approved by the Department. 10
SCREENINGS, COMPREHENSIVE NEEDS ASSESSMENT AND REASSESSMENT CHC-MCOs must screen each new participant who is not NCFE within 90 days of the start date of CHC in the zone. This requirement is separate from the assessment of those with LTSS or other special health needs. The CHC-MCO must conduct a comprehensive needs assessment of every participant who is determined NFCE. Information from the InterRAI Home Care tool is used to validate NFCE status. If the participant has not been determined NFCE, the CHC-MCO must conduct a comprehensive assessment when the participant makes a request, self-identifies as needing LTSS, or if either the CHC-MCO or the independent enrollment broker (IEB) identifies that the participant has unmet needs, service gaps or a need for service coordination. 11
COMPREHENSIVE NEEDS ASSESSMENT AND REASSESSMENT The CHC-MCO must complete an in-person comprehensive needs assessment in accordance with the following time frames: For NCFE participants who are not receiving LTSS on their enrollment date: no later than 5 business days from start date. For dually eligible participants identified by the IEB as having a need for immediate services: no later than 5 business days from the start date. For participants who are identified as having unmet needs, service gaps, or a need for service coordination: no later than 15 business days from the date the CHC-MCO is aware of the unmet needs, service gaps, or need for service coordination. 12
COMPREHENSIVE NEEDS ASSESSMENT AND REASSESSMENT Initial Needs Assessment The interRAI Home Care tool has replaced the CMI in the needs assessment process. The tool provides a determination of care needs to assist in the service planning process. The interRAI Home Care assessment data flows back into the Pennsylvania Individualized Assessment (PIA) system for long-term storage. Reassessments MCO is responsible for annual interRAI Home Care re-assessments and change in condition assessments. PIA extracts Functional Eligibility Determination (FED) weighted question responses from the interRAI Home Care tool assessment and re-calculates FED recommendation Aging Well PA reviews reassessments for discrepancies to ensure the validity 13 and appropriateness of the results.
COMPREHENSIVE NEEDS ASSESSMENT AND REASSESSMENT AT LEAST EVERY 12 MONTHS The CHC-MCO must conduct a comprehensive needs reassessment of NFCE participants no more than 12 months following the most recent prior comprehensive needs assessment or comprehensive needs reassessment unless a trigger event occurs. Trigger events include, but are not limited to: A significant health care event to include, but not be limited to: a hospital admission, a transition between health care settings, or a hospital discharge. A change in functional status. A change in caregiver or informal support status, if the change impacts one or more areas of health or functional status. A change in the home setting or environment, if the change impacts one or more areas of health or functional status. 14
COMPREHENSIVE NEEDS ASSESSMENT AND REASSESSMENT Through the comprehensive needs assessment and reassessment, the CHC-MCO must assess a participant’s physical and behavioral health, as well as social, psychosocial, environmental, caregiver, LTSS and other needs. Preferences, goals, housing, and informal supports are also assessed. If, after conducting the comprehensive needs assessment, the CHC-MCO determines that a participant who has not been determined NFCE has a need for LTSS, the CHC-MCO shall refer the participant for long-term care functional eligibility determination. The CHC-MCO must abide by the eligibility determination entity’s decision as to the need for nursing facility and long-term care services. 15
PERSON-CENTERED SERVICE PLAN (PCSP) The comprehensive needs assessment underwrites the person-centered planning process. The PCSP must address how the participant’s physical, cognitive, and behavioral health needs will be managed, including how Medicare coverage (if the participant is dually eligible) will be coordinated and how the participant’s LTSS services will be coordinated. The holistic PCSP will include both the care management plan and the LTSS plan. 16
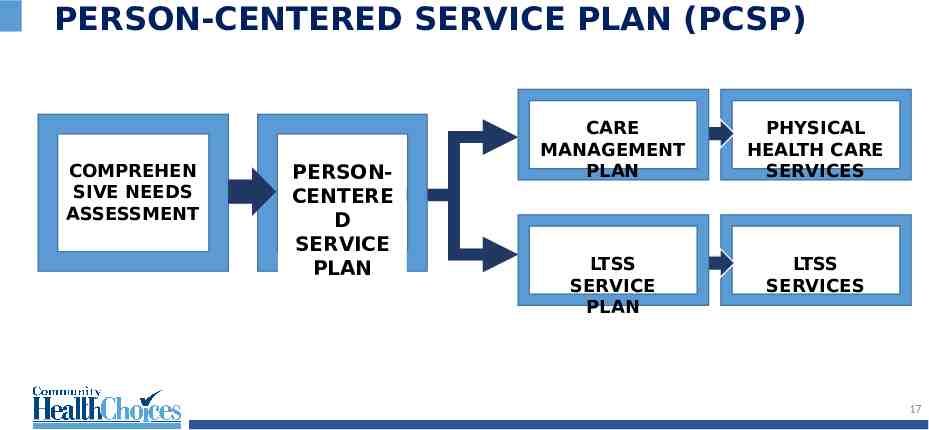
PERSON-CENTERED SERVICE PLAN (PCSP) COMPREHEN SIVE NEEDS ASSESSMENT PERSONCENTERE D SERVICE PLAN CARE MANAGEMENT PLAN PHYSICAL HEALTH CARE SERVICES LTSS SERVICE PLAN LTSS SERVICES 17
PERSON-CENTERED SERVICE PLAN (PCSP) CARE MANAGEMENT PLAN A care management plan is used to identify and address how the participant’s physical, cognitive, and behavioral health care needs will be managed, and will include, but will not be limited to: Active chronic problems, current non-chronic problems, cognitive needs, and problems that were previously controlled (classified as maintenance care) but have been exacerbated by disease progression or other intervening conditions Current medications All services authorized and the scope and duration of the services authorized, including any services that were authorized by the CHC- MCO since the last PCSP was finalized that need to be authorized moving forward The CHC-MCO must make available care management to all participants 18
PERSON-CENTERED SERVICE PLAN (PCSP) CARE MANAGEMENT PLAN A schedule of preventive-service needs or requirements Disease management action steps Known needed physical and behavioral health care and services All designated points of contact; the participant’s authorizations of who may request and receive information about the participant’s services How the service coordinator will assist the participant in accessing services identified in the PCSP How the CHC-MCO will coordinate with the participant’s Medicare, Veterans, BHMCO, and other health insurers and other supports 19
PERSON-CENTERED SERVICE PLAN (PCSP) LTSS SERVICE PLAN A LTSS service plan must identify and address how LTSS needs will be met and how services will be provided in accordance with the PCSP. The LTSS service plan must include the following: All LTSS services necessary to support the participant in living as independently as possible and remaining as engaged in his/her community as possible. For the needs identified in the comprehensive needs assessment, the interventions to address each need or preference, reasonable long-term and short-term goals, the measurable outcomes to be achieved by the interventions, the anticipated timelines in which to achieve the desired outcomes, and the staff responsible for conducting the interventions and monitoring the outcomes 20
PERSON-CENTERED SERVICE PLAN (PCSP) LTSS SERVICE PLAN Potential problems that can be anticipated, including risks and how these risks can be minimized to foster the participant’s maximum functioning level of well-being Participant decisions around self-directed care, and whether the participant is participating in participant-direction Communications plan How frequently specific services will be provided How -- or if -- technology and telehealth will be used Participant choice of providers and service coordinators 21
PERSON-CENTERED SERVICE PLAN (PCSP) LTSS SERVICE PLAN Participant’s available, willing, and able informal support network and services Participant’s need for and plan to access community resources, non-covered services and other supports, including any reasonable accommodations How to accommodate preferences for leisure activities, hobbies, and community engagement Any other needs or preferences of the participant Participant’s goals for the least restrictive setting possible; if he or she is being discharged or transitioned from an inpatient setting. 22
PERSON-CENTERED SERVICE PLAN (PCSP) LTSS SERVICE PLAN The process for reporting abuse, neglect and exploitation The process for reporting suspected fraud and abuse Individualized back-up plans The person(s) and providers responsible for specific interventions or services How the CHC-MCO will coordinate with the participant’s Medicare, Veterans Benefits, BH-MCO, other health coverage insurers, and other supports Participant’s employment and educational goals 23
PERSON-CENTERED SERVICE PLAN (PCSP) The PCSP must specify the need for referrals and the need for assistance from the service coordinator in obtaining referrals. To the extent that the primary care practitioner is part of the PCSP development, the PCSP must also articulate referrals that the service coordinator will enter in the appropriate systems. The PCSP must consider both in- and out-of-network covered services to support the individual in the environment of his/her choice, as well as caregivers’ support needs 24
PERSON-CENTERED SERVICE PLAN (PCSP) PCSPs must be completed no more than 30 days from the date that the comprehensive needs assessment or reassessment is completed. PCSPs must be developed by the service coordinator, the participant, the participant’s representative, and the person-centered planning team. Participants may appeal part or all of their service plan as provided through the complaint, grievance and DHS fair-hearing processes. 25
PERSON-CENTERED PLANNING TEAM (PCPT) CHC requires a PCPT approach as part of the service planning and servicecoordination processes for participants who require LTSS. The CHC-MCOs may also include the PCPT approach as part of the overall care coordination approach for participants who do not require LTSS. The PCPT approach must be person-centered and must take into account all goals and requirements of CHC. Team members may include participants, their caregivers, primary care physicians, specialists, behavioral health providers, direct care workers, and any other individual involve in the participant’s service planning. 26
PARTICIPANT-DIRECTED SERVICES Participant-directed services, including Services My Way, will continue, and CHCMCOs will offer the option to all participants receiving HCBS. Just like today, the CHC-MCO’s SCs will work with the participant to create an individualized service plan regarding type, scope, amount, duration and frequency of services needed. The SC will monitor the provision and utilization of services to ensure the participant’s health and welfare. The CHC-MCOs are required to comply with state and federal regulations including the Department of Labor Fair Labor Standards Act regulations at 29 CFR Part 552 requirements related to minimum wage, overtime pay, and travel time. Just like today, the SC will work with the individual if overtime pay requires a modification to the individual’s budget. All participants who are transitioning to the CHC waiver and who are utilizing a PDS model will transition to monthly authorizations. 27
PARTICIPANT-DIRECTED SERVICES Financial Management Services (FMS) will continue. The CHC-MCOs are required to establish agreements and cooperate with the Commonwealth-procured Fiscal/Employer Agent (F/EA) in order that necessary FMS services are provided to participants. The F/EA will continue to perform the same functions as today: Prepare and distribute payroll and address federal, state, and local employment tax; labor, and workers compensation insurance rules; and other requirements that apply when the participant functions as the employer of his or her workers Make financial transactions on behalf of the participant Generate reports for participants, CHC-MCOs and OLTL 28
NURSING HOME TRANSITION (NHT) NHT is an administrative role for the CHC-MCOs. CHC-MCOs must provide NHT activities to participants residing in nursing facilities who express a desire to move back to their homes or other community-based settings. The CHC-MCO must provide NHT activities using appropriately qualified staff, whether employed by or under contract with the CHC-MCO. Services coordinators will participate in these activities, although the CHC-MCOs may have dedicated staff focused on the responsibilities of this role. 29
NURSING FACILITY TO HCBS TRANSITION New process for the County Assistance Office (CAO) to expedite financial eligibility determinations for applicants transitioning from Nursing Facilities to Home and Community Based Services (HCBS). Effective February 19, 2019 the CAO will process waiver applications 2 weeks prior to NF discharge. Allows participants to make an informed choice and safe discharge plan. 30
COORDINATION WITH NON-MEDICAID SERVICES For a participant who is receiving home- and community-based services other than through a HCBS waiver on the participant’s start date, the CHC-MCO service coordinators must coordinate the participant’s transition into CHC with entities that are providing care or service coordination to the participant at the time of their CHC enrollment. The CHC-MCO service coordinators must coordinate with entities providing these services outside of CHC including, but are not limited to, the Act 150 program, the OPTIONS program or OMAP’s Special Needs Unit. 31
MONITORING MONITORING MISSED SERVICES AND PERSON-CENTERED SERVICE PLANS OLTL has developed monitoring reports to capture LTSS service plan changes, missed services, service denial notices, and complaints and grievances through the continuity of care period and ongoing after the continuity of care period ends. These reports include: OPS 3 & 4 – Complaints and Grievances OPS 8 – Services Not Delivered OPS 21 – Person-Centered Service Plan Changes QMUM 7 – Denial Log These reports help OLTL to assure participants are receiving services and to help ensure participant health and safety. Service coordinators play a critical role in providing information or taking follow up steps to the CHC-MCOs to assist in monitoring efforts. OLTL staff monitor the reports and addresses concerns with the CHC-MCOs. The MCOs may request additional information from service coordinators to assist in responding to OLTL requests. 32
ELECTRONIC VISIT VERIFICATION (EVV) WHY IS EVV BEING IMPLEMENTED? The 21st Century Cures Act requires electronic visit verification (EVV) for Medicaid covered personal care services by January 1, 2019 and home health care services by January 1, 2023 (Sec. 207). The EVV system must verify and record electronically (for example, through a telephone or computer-based system): the type of service performed; the individual receiving the service; the date of the service; the location of the service; and the time the service begins and ends. OLTL waiver services included in the initial implementation of EVV include: Personal Assistance Services (Agency and Participant-Directed Model) Participant-Directed Community Supports Respite (unlicensed settings only) 33
ELECTRONIC VISIT VERIFICATION (EVV) HOW IS THE DEPARTMENT DEVELOPING THE EVV APPROACH? The Department solicited input from participants, family caregivers, provider agencies, and individuals who furnish personal care services or home health care services, managed care organizations, and other stakeholders on the current use of EVV in the commonwealth and the impact of EVV implementation. The Department intends to implement the EVV requirements so that the system is minimally burdensome and will take into account the input from stakeholders. DHS is working with vendors to develop an EVV system and aggregator that will integrate with PROMISe, our existing Medicaid Management Information System. CHC-MCOs are required to have EVV systems that comply with this requirement. Providers may use other EVV vendors/systems (Alternate EVV). Alternate EVV systems will need to capture the six required items under the Cures Act and will need to meet DHS system data requirements. 34
ELECTRONIC VISIT VERIFICATION (EVV) WHEN WILL THE DEPARTMENT IMPLEMENT EVV? May 2019 – FAQ document, Alternative EVV Technical Specifications, and DHS Addendum to be distributed to providers. August-October 2019 – Provider training to be offered to providers choosing to use the DHS EVV system with phased in system use. Training will continue to be offered through full implementation. At this time, providers using Alternative EVV systems must work with the DHS EVV vendor, Sandata, to ensure their system can integrate with the EVV Aggregator. September-October 2019 – Go live and soft launch of DHS EVV system. January 2020 – Full implementation of the system as required by the 21st Century Cures Act. Additional EVV implementation information will be posted to the DHS website as it becomes available: http://www.dhs.pa.gov/provider/billinginformation/electronicvisitverification/index.htm Additional EVV questions can be sent to [email protected] 35
CHC PROVIDERS & EVV Providers Serving Participants in an Active CHC Zone (Southwest or Southeast) Providers in CHC will have the option to use the MCO’s internal EVV system. A CHC-participating provider with their own internal EVV system must work with each contracted MCO to ensure the provider’s system is able to send information to the MCO’s system. Providers should begin discussing training and system options with their contracted MCO(s) in order to implement EVV by October 2019. Providers Serving Participants in the Phase 3 Region of CHC (Lehigh/Capital, Northeast, and Northwest) Includes providers currently serving participants in Aging, Attendant Care, and Independence waivers Providers who will be participating in CHC will have the option to use the MCO’s internal EVV system. A CHC-participating provider with their own internal EVV system must work with each contracted MCO to ensure the provider’s system is able to send information to the MCO’s 36 system.
OLTL FFS PROVIDERS & EVV Providers Serving Participants in the OBRA Waiver or Act 150 Program Providers participating in the OBRA waiver or Act 150 program will have the option to use the DHS system or use their own internal system. Providers who choose to use the DHS system must participate in training in order to gain access to the system when it is implemented. Providers who choose to use their own internal system must allow at least 60 days before soft launch to complete certification and testing with the DHS EVV vendor, Sandata. 37
LESSONS LEARNED FROM THE SW AND SE IMPLEMENTATIONS Earlier training for external service coordinators both to support the continuity of care period and to clarify the role and function of the service coordinator in CHC Ongoing and improved communication with the CHC-MCOs and external service coordinators Data clean-up and standardization in the legacy case management systems (HCSIS/SAMS) Earlier user account set-up in the CHC-MCO systems Earlier and more rapid change of EIM user account information to reflect new relationship in CHC with the CHC-MCOs An evaluation and augmented training of both internal and external service coordinator understanding of the person-centered planning process Service coordinator participation in data clean-up and file transfer efforts Encourage proactive redeterminations prior to the implementation of a CHC phase Education of service coordinators about participant transitions between CHCMCOs and with significant provider changes 38
SERVICE COORDINATOR TESTIMONIAL 39
MANAGED CARE ORGANIZATIONS The selected offerors were announced on August 30, 2016. www.AmerihealthCaritasCHC.com www.PAHealthWellness.com www.upmchealthplan.com/chc 40
CHC-MCO APPROACH TO SERVICE COORDINATION Enrollment through the continuity of care period Service coordinator training including training on systems and the personcentered planning process Systems access Approaches to comprehensive needs assessment, person-centered service planning, and NHT Approaches to care management and LTSS management 41
QUESTIONS 42