REGIONAL OUTCOMES FOR SURGICAL MANAGEMENT OF EARLY STAGE CERVICAL
25 Slides1.29 MB
REGIONAL OUTCOMES FOR SURGICAL MANAGEMENT OF EARLY STAGE CERVICAL CANCER Dr S Coleridge Clinical Fellow Gynaeoncology Musgrove Park Hospital, Taunton ST6 OOPR
WHY? LACC data presented Consensus to inform women about to undergo a radical hysterectomy of unpublished trial findings Informed consent Montgomery ruling Women want to know why we are recommending a particular treatment Can provide local data to help inform shared decision making
RANDOMISED CONTROLLED TRIAL VS RETROSPECTIVE COHORT Randomly assign participants to control group (open surgery) or intervention group (minimal access surgery) Gold standard of evidence based medicine Minimise bias Control for confounding factors Observational Middle of the hierarchy of evidence Useful to inform clinical practice
LAPAROSCOPIC RADICAL HYSTERECTOMY
LACC HYPOTHESIS Minimal access surgery is cost effective, improves QoL and pelvic floor function with equivalent overall survival to open surgery Decreased treatment related morbidity (8%) Shorter hospital stay Less post op pain Reduced analgesic consumption Equivalence measured by disease free survival(DFS) within 7.2% of open DFS rate
LAPAROSCOPIC RADICAL HYSTERECTOMY “I'm 5 weeks post op now and feel great. I'm starting back to work next week. My incision sites are still a little sore” “I wanted to say that I felt keyhole surgery was right option for me as the recovery time is quicker and this was important for me as a single parent of 3 kids and limited family support”
OPEN ABDOMINAL HYSTERECTOMY “It's taken 4 months to start to feel ok-ish” “I'd say for anyone having the abdominal surgery.this is a hard recovery but it does get better, from speaking to people having had this op it does take a couple of months more than keyhole to get to the milestones they give you. Take it steady!”
INCLUSION CRITERIA FIGO stage 1a1 with LVSI 1a2 1b1 Histological subtype Adenocarcinoma Squamous cell carcinoma Adenosquamous carcinoma Tumour size 4cm
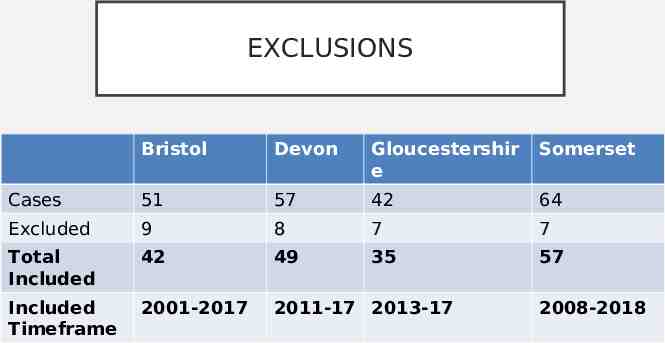
EXCLUSIONS Bristol Devon Gloucestershir e Somerset Cases 51 57 42 64 Excluded 9 8 7 7 Total Included 42 49 35 57 Included Timeframe 2001-2017 2011-17 2013-17 2008-2018
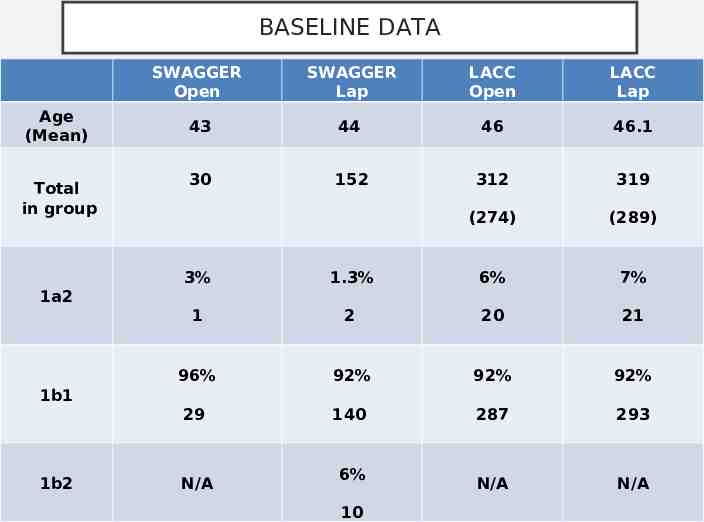
BASELINE DATA Age (Mean) Total in group SWAGGER Open SWAGGER Lap LACC Open LACC Lap 43 44 46 46.1 30 152 312 319 (274) (289) 3% 1.3% 6% 7% 1 2 20 21 96% 92% 92% 92% 29 140 287 293 N/A N/A 1a2 1b1 1b2 N/A 6% 10
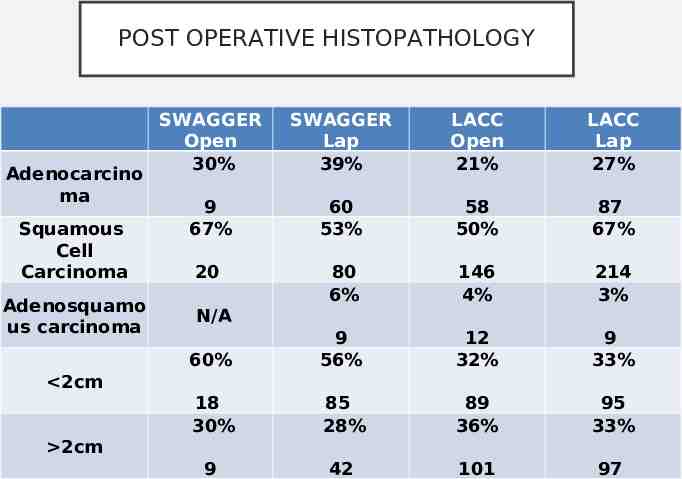
POST OPERATIVE HISTOPATHOLOGY Adenocarcino ma Squamous Cell Carcinoma Adenosquamo us carcinoma SWAGGER Open 30% SWAGGER Lap 39% LACC Open 21% LACC Lap 27% 9 67% 60 53% 58 50% 87 67% 20 80 6% 146 4% 214 3% 60% 9 56% 12 32% 9 33% 18 30% 85 28% 89 36% 95 33% 9 42 101 97 N/A 2cm 2cm
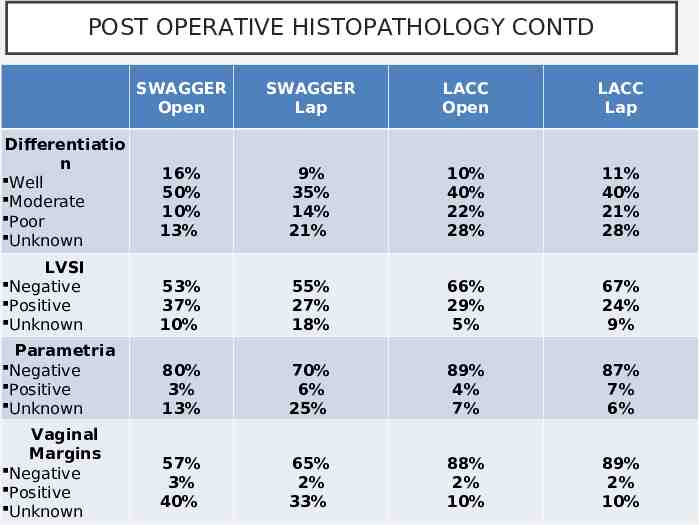
POST OPERATIVE HISTOPATHOLOGY CONTD SWAGGER Open SWAGGER Lap LACC Open LACC Lap 16% 50% 10% 13% 9% 35% 14% 21% 10% 40% 22% 28% 11% 40% 21% 28% LVSI Negative Positive Unknown 53% 37% 10% 55% 27% 18% 66% 29% 5% 67% 24% 9% Parametria Negative Positive Unknown 80% 3% 13% 70% 6% 25% 89% 4% 7% 87% 7% 6% 57% 3% 40% 65% 2% 33% 88% 2% 10% 89% 2% 10% Differentiatio n Well Moderate Poor Unknown Vaginal Margins Negative Positive Unknown
POST OP CHEMORADIOTHERAPY LACC criteria - LVSI / tumour size / stromal invasion
SURGERY VS. CHEMORADIOTHERAPY “I went on to have chemo-rads anyway and have been cancer-free ever since, but it is my firm belief that the outcome would have been the same without the unnecessary loss of body parts. But in all honesty, I could have done without losing the top 50% of my vagina”
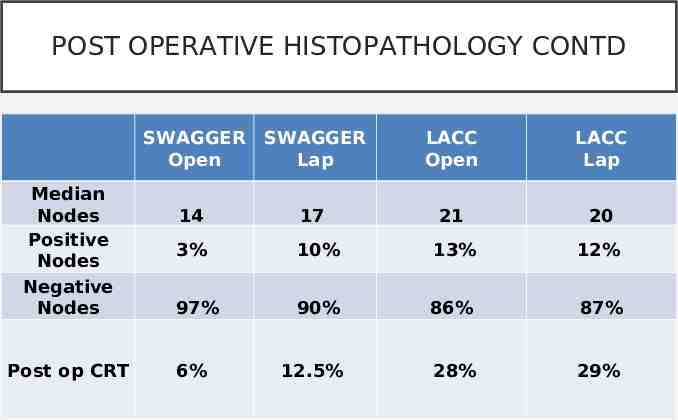
POST OPERATIVE HISTOPATHOLOGY CONTD SWAGGER Open SWAGGER Lap LACC Open LACC Lap 21 20 Median Nodes Positive Nodes Negative Nodes 14 17 3% 10% 13% 12% 97% 90% 86% 87% Post op CRT 6% 12.5% 28% 29%
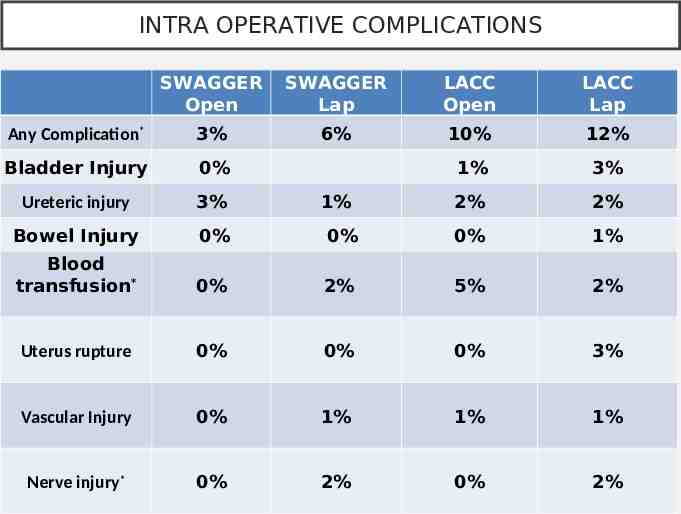
INTRA OPERATIVE COMPLICATIONS SWAGGER Open SWAGGER Lap LACC Open LACC Lap Any Complication* 3% 6% 10% 12% Bladder Injury 0% 1% 3% Ureteric injury 3% 2% 2% Bowel Injury 0% 0% 0% 1% Blood transfusion* 0% 2% 5% 2% Uterus rupture 0% 0% 0% 3% Vascular Injury 0% 1% 1% 1% Nerve injury* 0% 2% 0% 2% 1%
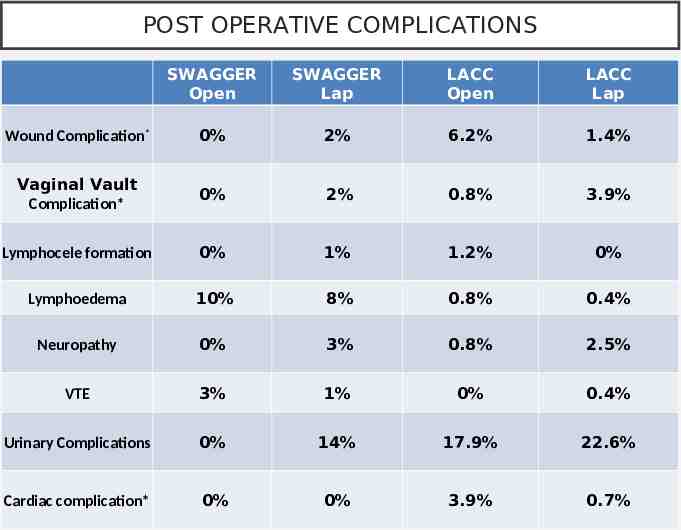
POST OPERATIVE COMPLICATIONS SWAGGER Open SWAGGER Lap LACC Open LACC Lap Wound Complication* 0% 2% 6.2% 1.4% Vaginal Vault Complication* 0% 2% 0.8% 3.9% Lymphocele formation 0% 1% 1.2% 0% Lymphoedema 10% 8% 0.8% 0.4% Neuropathy 0% 3% 0.8% 2.5% VTE 3% 1% 0% 0.4% Urinary Complications 0% 14% 17.9% 22.6% Cardiac complication* 0% 0% 3.9% 0.7%
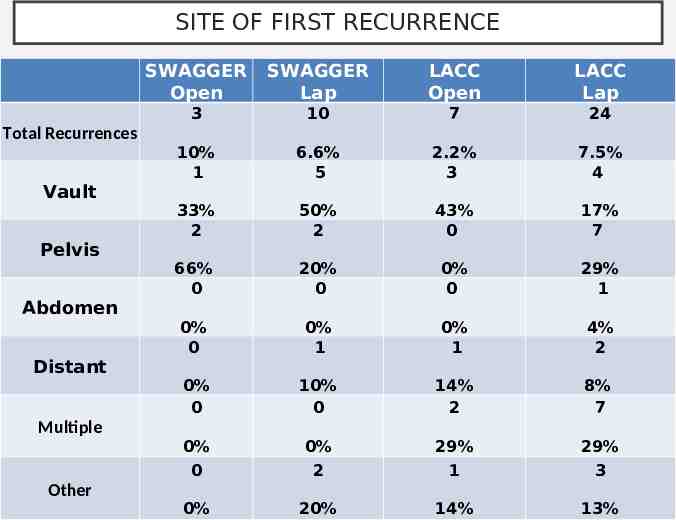
SITE OF FIRST RECURRENCE Total Recurrences Vault Pelvis Abdomen Distant Multiple Other SWAGGER Open SWAGGER Lap LACC Open LACC Lap 3 10 7 24 10% 1 6.6% 5 2.2% 3 7.5% 4 33% 2 50% 2 43% 0 17% 7 66% 0 20% 0 0% 0 29% 1 0% 0 0% 1 0% 1 4% 2 0% 0 10% 0 14% 2 8% 7 0% 0% 29% 29% 0 2 1 3 0% 20% 14% 13%
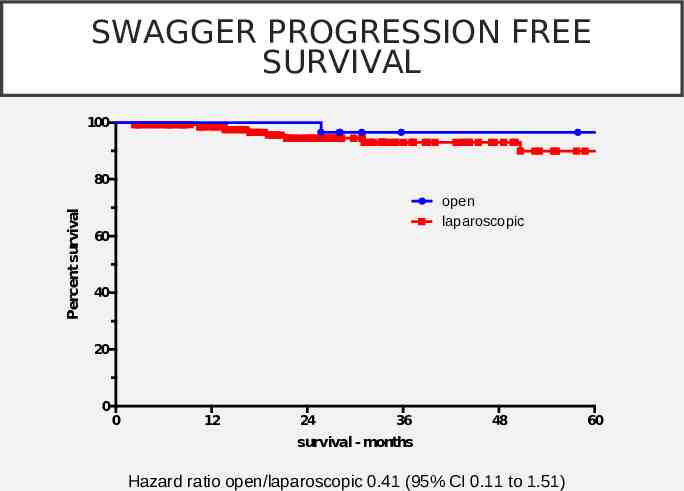
SWAGGER PROGRESSION FREE SURVIVAL Progression free survival (months) 100 Percent survival 80 open laparoscopic 60 40 20 0 0 12 24 36 48 survival - months Hazard ratio open/laparoscopic 0.41 (95% CI 0.11 to 1.51) 60
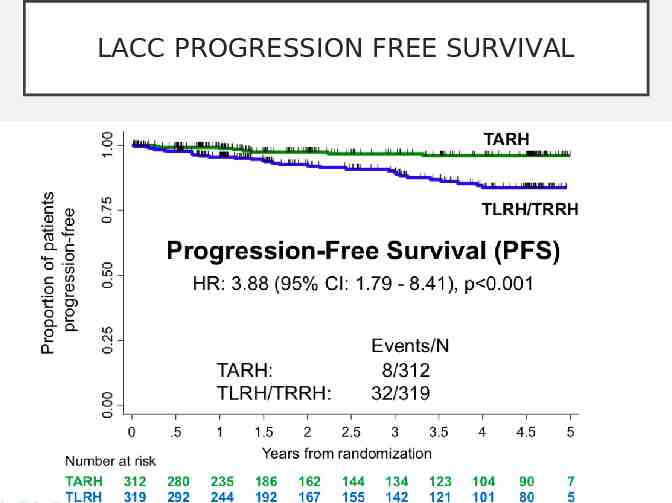
LACC PROGRESSION FREE SURVIVAL
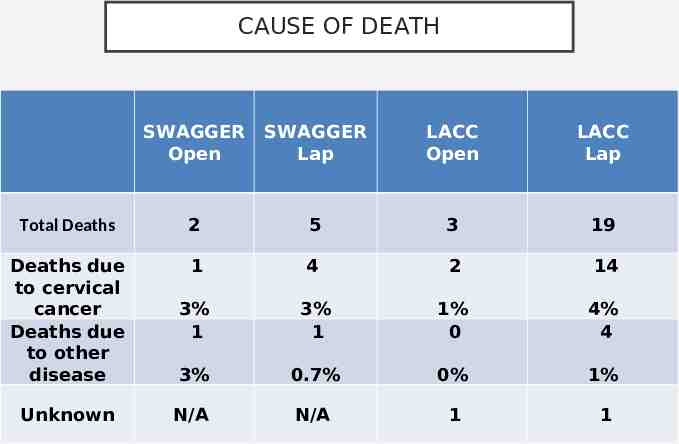
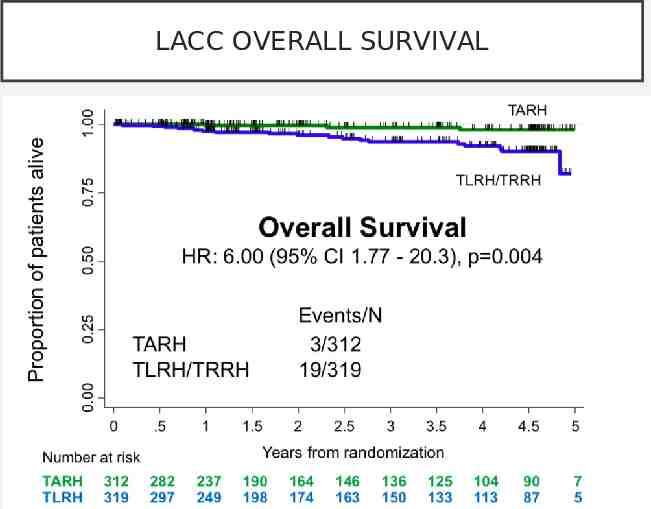
CAUSE OF DEATH SWAGGER Open SWAGGER Lap LACC Open LACC Lap Total Deaths 2 5 3 19 Deaths due to cervical cancer Deaths due to other disease 1 4 2 14 3% 1 3% 1 1% 0 4% 4 3% 0.7% 0% 1% Unknown N/A N/A 1 1
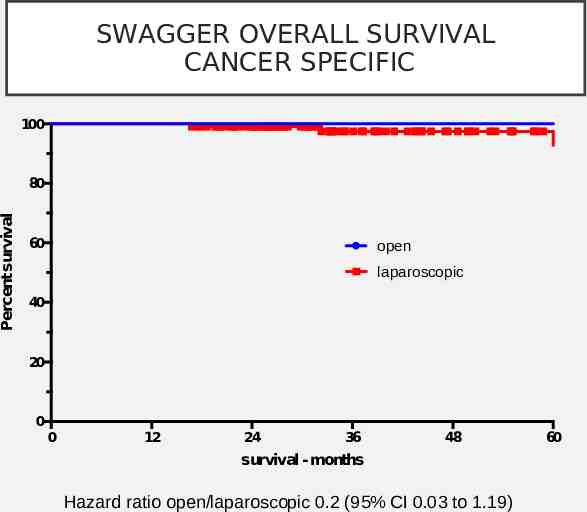
SWAGGER OVERALL SURVIVAL CANCER SPECIFIC Cancer specific survival (months) 100 Percent survival 80 60 open laparoscopic 40 20 0 0 12 24 36 48 survival - months Hazard ratio open/laparoscopic 0.2 (95% CI 0.03 to 1.19) 60
LACC OVERALL SURVIVAL
GOING FORWARD What Next?
THANK YOU Mr Milliken Miss Morrison Miss Newton Mr Rolland Mr Hannemann