Pain Management Strategies for Primary Care David Buyck, Ph.D.





















43 Slides400.17 KB
Pain Management Strategies for Primary Care David Buyck, Ph.D. Sarah Lucas Hartley, Ph.D. Salem Veterans Administration Medical Center 1
Learning Objectives Theoretical and historical influences. Knowledge of assessment strategies and criteria. Familiarity with treatment strategies. 2
Defining Chronic Pain Chronic Pain Acute Pain Physical pain of a Physical pain of duration greater than 6 months a duration less than 6 This presentation months will focus on Some utility of Chronic Pain here but less than for Chronic 3
Categories of Chronic Pain Chronic recurrent pain – Benign condition – Intense pain alternating with pain-free periods – E.g., Headaches, endometriosis Chronic intractable benign pain – – – – – Benign condition Persistent - no pain free periods Intensity may vary Objective medical findings often limited E.g., Back pain Chronic progressive pain – Malignant condition – Continuous - increasing intensity – E.g., Cancer and rheumatoid arthritis 4
Prevalence and Incidence 10-15% of Americans are disabled due to back pain alone (DSM-IV). 70,000,000 Americans will seek pain treatment in a given year (Gatchel & Weisberg, 2000). 4 out of 5 clinicians agree that you shouldn’t trust any of these statistics. 5
Pain Prevalence in the VA 50% of the VA population suffers CP. Prevalence is growing: – 42.7% of OIF/OEF enrollees report chronic pain. – Most frequent OIF/OEF diagnoses are diseases of the Musculoskeletal system. 6
Co-morbidity of Chronic Pain & Mental Illness 15.4% Psychiatric Illness base rate. 51-58% Rate of Psychiatric Illnesses among patients with CP. 4X the prevalence of general population. In the VA, over 80% of PTSD patients have co-morbid CP. 20% of patients on VA SUD inpatient programs have CP. 7
.we are not ourselves when nature, being oppressed, commands the mind to suffer with the body. Shakespeare, King Lear 8
Costs to Patients and Society Often compromises all aspects of life Elusive quest for relief Demoralization, helplessness, hopelessness Grief Taxes relationships Frustration for health care providers Chronic pain is incompatible with societal myths Perpetuation of stereotypes Addiction Opportunity costs to GNP Often given severely limited resources due to surreptitious or inadvertent ageism and fear. 9
Historical Influences Aristotle (384-322 BC) DeAnima- “Pain is a quality of the soul.” 1640’s Renaissance – Descartes dualistic. 1895 – Freud psychosomatics. 10
Iceman of the Alps “Utze” Oldest, best preserved corpse. 5300 years old. Daniel Carr, M.D. & A.P.S. 11
Emergence of Psychosomatic Medicine 1956 – Beecher- soldiers & civilians. 1965 - gate control theory - Melzack & Wall. The health belief model (US Public Health Service, Late 50’s ) Voluntary control of ANS (i.e., Biofeedback)- Basmajian (1963); Miller (1969). 12
Emergence of Psychosomatic Medicine 1976 - Operant conditioning - Fordyce – model of “pain behavior” – “activity intolerance” Cognitive-behavioral, importance of: – appraisal, – beliefs and – expectations. 1999 – Uhl, Sora & Wang –identified “pain sensitivity gene.” 13
Gate Control Theory Ronald Melzack & Patrick Wall (1965) Diverse factors in pain perception Importance of CNS & psychological factors Melzack’s current research: “body-self neuromatrix” Cortical Neuroplasticity (Apkarian, Bushnell, Merzenich, Zhou) 14
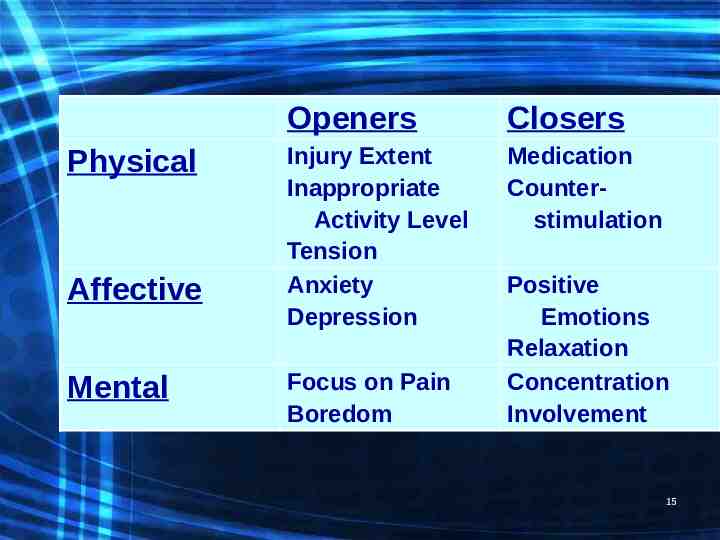
Openers Closers Injury Extent Medication Physical Controlling the Gate Affective Mental Inappropriate Activity Level Tension Anxiety Depression Focus on Pain Boredom Counterstimulation Positive Emotions Relaxation Concentration Involvement 15
The 4-Stage Integrated Model (Price, 1988; Wade, Dougherty, & Archer, 1996) 16
Why Integrate – 50% of the VA population suffers CP. – Primary Care handles pain management longitudinally. – Behavioral aspects around Pain Management: Always #1 PC need on NGP and needs assessments – No-shows for ancillary referrals are high. 17
MHI Pain Strategy – – – – No referral needed MHI Screens/Triages – Open-Access Moves to group/BMed in Same Week MI/Integrated support around adherence issues 18
Rules for Group Inclusion Patients must: Express willingness and motivation to attend Be free of active substance or alcohol abuse or dependence Be in concurrent, active, effective treatment if they meet criteria for any mental disorder (including personality disorders) Be free of active current psychosis, mania, suicidal or homicidal ideation. These conditions will need to be stabilized in specialty mental health care prior to pain group admission Limitations of treatment: It can be helpful to inform patients during the screening encounter that we are not prescribers and do not offer medications, surgeries, and that we cannot influence medical decisions. 19
Chronic Pain Manageme nt Group Pain Psychology Triage in Primary Care MHI Managed MHI Primary Care Provider 20
Pain Psychology Triage in Primary Care PCP MHI Chron ic Pain Group MHI Man aged 21
Key MI Issues – Agenda setting/active listening. – referral may reinforce fear that provider believes its “all in my head.” – Convey that pain influences most aspects of life. – Full psychophysiological understanding. – “Behavioral medicine” vs. “Psychological evaluation” – Stress interferes with physical recovery. – Limitations of treatment. 22
The Waddell Signs Tail bone pain in a patient with a back injury. Whole leg pain except diabetic or alcoholic neuropathy. Whole leg numbness, except in diabetic or alcoholic neuropathy. Whole leg giving way. Absence of pain free periods. Intolerance and reactions to treatment. Hospital admission for simple low back pain. 23
Waddell Signs Waddell signs “do not directly measure faking, but point to psychological suffering or unconscious neurotic behavior. If patients with high Waddell scores do not receive psychological intervention, they probably will not improve”. - Waddell 24
Signs of Narcotic Dependence & “Drug Seeking” Multiple lost or stolen scripts Multiple pharmacies and/or physician prescribers Multiple dose escalations despite adverse effects Focused only on medication types or doses Unwilling to consider or try non-opioid therapy Consistently running out of medications early Frequent calls, especially after hours Agitation at providers over medications Illicit drugs on screens Injecting oral narcotics Prescription forgery Steeling or borrowing drugs from others Selling prescription drugs 25
Signs of Pseudo-addiction (seeking adequate pain relief) Escalating doses without improved analgesia High doses without concern of side-effects Withdrawal symptoms Hoarding when symptoms are reduced Acceptance of non-opioid regimens Frequent request to modify regimen to produce relief Requesting specific narcotics Dose escalation without physician consent once or twice 26
Psychological Goals in Pain Treatment Increase coping with pain sensation Increase coping with threat to functioning Reduce associated emotional distress 27
Typical CBT Pain Format Keefe, Jacobs & Underwood-Gordon (1997) 1. Educational component. 2. Recognizing & challenging irrational beliefs. 3. Instruction in behavioral skills. 4. Identification of & planning for high-risk situations. 5. Decision making & problem solving re: employment, relationships, etc. 28
Our Group Format 10 general topics – – – – – – – – – – Pacing Becoming more active Re-thinking & outsmarting pain Relaxation & stress management Getting in better shape Re-claiming recreation & work Dealing with family and friends Healthy habits Social activity Working with health-care providers 29
Psychological Goals in Pain Treatment Increase coping with pain sensation Increase coping with threat to functioning Reduce associated emotional distress 30
Assumptions of CBT Turk & Rudy (1989); Bradley (1996) Active processing of internal & environmental events Thoughts behavior through emotional, physiological responses Behavior environment Treatment must address emotional, cognitive, behavioral and physiological Active participation from patient 31
Typical CBT Pain Format Keefe, Jacobs & Underwood-Gordon (1997) 1. Educational component. 2. Recognizing & challenging irrational beliefs. 3. Instruction in behavioral skills. 4. Identification of & planning for high-risk situations. 5. Decision making & problem solving re: employment, relationships, etc. 32
Educational Component Assess what they already know. “Take ‘em where they’re at.” Pain’s purpose. – Example of Congenital analgesia. Use analogies (nerves-wires). 33
Recognizing & Challenging Irrational Thoughts Beliefs – “fix me doc.” Automatic reactive patterns. – E.g., Flare-up anger, tension, resentment. Motivational attitudes. – Internal vs external LOC. – Stages of change (Prochaska & DiClemente, 1982; Jensen, Neilson, and Kerns, 2003; Glenn, B. & Burns, J, 2003). Reframing – “It’s not in your head, but you can use your head to help deal with it.” 34
Instruction in Behavioral Skills Relaxation Imagery-hypnotic analgesia Distraction Listing pain behaviors & responses 35
Instruction in Behavioral Skills Exercise Pacing Assertiveness Practiced in session then as homework Self-monitoring & self-reinforcement 36
Planning for High-risk Situations Flare-up plans (pre-emptive analgesia) Work & home stressors Emotional upsets Relapse prevention – Teach to recognize early signs (depression, anxiety, pain, diet, exercise) – Rehearsal of responses – Self-reinforcement training 37
Decision Making & Problem Solving Indicators of poor problem solving. – Generation of few possible solutions. – Suggested solutions don’t include social supports. – Inaccurate expectations of probable consequences. 38
Decision Making & Problem Solving Steps for problem solving. – – – – – – – – Acknowledge & identify problem. Ask who owns the problem. Identify needs of those affected. Identify resources. Brainstorming. Evaluate options based on step 3. Implement an option. Evaluate outcome. 39
CBT Group Treatment Advantages – Fixed format – Social facilitation – “We are not alone” – Veteran phenomenon Disadvantages – Relatively inflexible – Crises more challenging – Not as individualized – Can be 40
The End 41
Transtheoretical Model 42
The Health Belief Model 43