Opioid Addiction and Medication–Assisted Treatment (MAT) Rob


58 Slides1.93 MB
Opioid Addiction and Medication–Assisted Treatment (MAT) Rob Campbell, MD, FACS, FASAM Clinical Faculty, University of Louisville, The Ohio State University, and Ohio Health Departments of Psychiatry Ohio University College of Medicine Wright State University College of Medicine Staff Psychiatrist Twin Valley Behavioral Health Columbus, Ohio
What is addiction? American Society of Addiction Medicine (ASAM): “A primary, chronic disease of brain reward, motivation, memory, and related circuitry," with a "dysfunction in the circuits" being reflected in an individual pathologically pursuing reward and/or relief by substance use and other behaviors.” DSM-5 uses the term "Opioid Use Disorder“ (OUD), the term which will be used throughout this presentation.
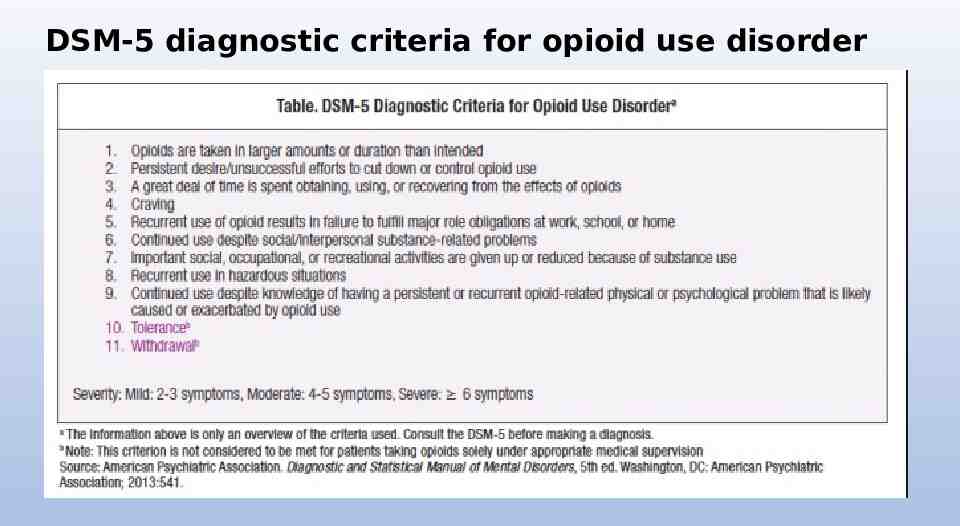
DSM-5 diagnostic criteria for opioid use disorder
Opioid overdose crisis Every day, more than 150 people in the United States die after overdosing on opioids. Misuse of and addiction to opioids—including prescription pain relievers, heroin, and synthetic opioids such as fentanyl—is a serious national crisis that affects public health as well as social and economic welfare. CDC : ”Total economic burden" of prescription opioid misuse alone in the United States is over 100 billion a year, including the costs of healthcare, lost productivity, addiction treatment, and criminal justice involvement.”
What do we know about the opioid crisis? Roughly 21 to 29 percent of patients prescribed opioids for chronic pain misuse them. Between 8 and 12 percent develop an opioid use disorder. An estimated 4 to 6 percent who misuse prescription opioids transition to heroin. About 80 percent of people who use heroin first misused prescription opioids. Opioid overdoses increased 30 percent from July 2016 through September 2017 in 52 areas in 45 states. The Midwestern region saw opioid overdoses increase 70 percent from July 2016 through September 2017. Opioid overdoses in large cities increased by 54 percent in 16 states.
What do we know about the opioid crisis? 2013 National Survey on Drug Use and Health: 4.5 million individuals in US are current (past month) nonmedical users of prescription opioids. 289,000 are current (past month) users of heroin. Leading causes of death in people using opioids for nonmedical purposes are overdose and trauma. Injection route use (IV or IM) increases risk of HIV and hepatitis exposure.
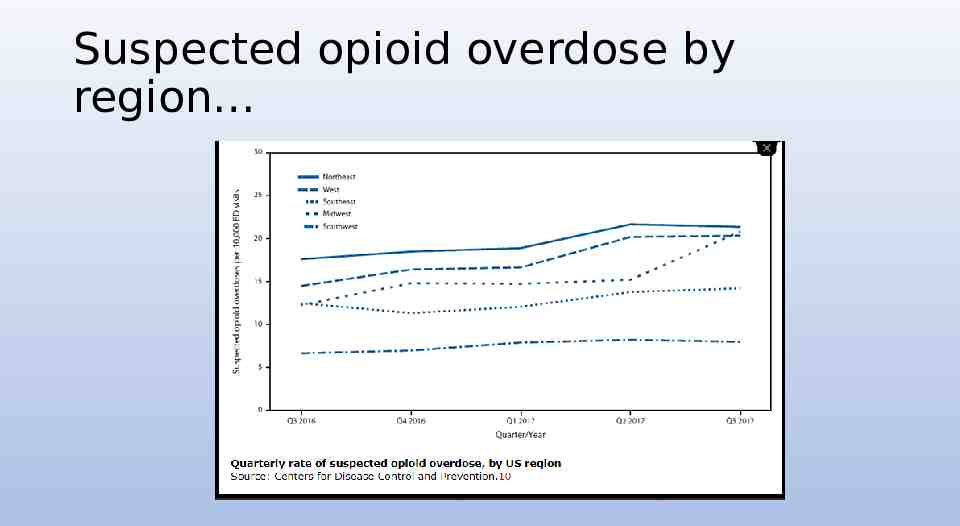
Suspected opioid overdose by region
Issues related to the opioid crisis Neonatal abstinence syndrome (NAS) Hepatitis C (HVC) HIV Life-threatening infections such as endocarditis
Brief Review of the Pharmacology Of Opioids: Opioid Receptors Opioid receptor agonists cause dopamine release in the nucleus accumbens. 3 opioid receptors in humans: mu (MOPr): encoded by the OPRM1 gene kappa (KOPr):encoded by the OPRK1 gene delta (DOPr): encoded by the OPRD1 gene Most clinically used opioid compounds, as well as medications with major use in addiction pharmacotherapy, methadone, and buprenorphine, respectfully, act primarily as agonists or partial agonists , at MOPr. Naloxone, naltrexone, and nalmefene act as MOPr antagonists and also have affinity at KOPr (acting as antagonists or potentially partial agonists). Naloxone is used primarily to reverse effects of opioid agonists mentioned above in specific clinical situations (e.g., overdose).
Main Opioid Compounds Encountered Clinically HEROIN: Derived from the natural alkaloid morphine, extracted from the opium poppy. Rapid onset of action and short half-life and is a frequent drug of abuse (it is also available for limited indications in some countries outside the united states). Prodrug, with active metabolites (primarily 6-acetylmorphine and morphine). Most potent when used intravenously but increasingly used intranasally and is also smoked in the free-base form.
Main Opioid Compounds Encountered Clinically CODEINE (3-methylmorphine): Derived from the opium poppy Used orally for mild-to-moderate pain, often co-formulated with acetaminophen. Due to the presence of acetaminophen (known as paracetamol in many countries outside the United States), abuse of such formulations carries a risk of hepatotoxicity. Codeine is less potent and efficacious than is morphine. Up to 15% is o-demethylated to morphine, the most active metabolite, which has 200 times greater affinity for the mu opioid receptor compared to codeine. Metabolism is primarily via CYP2D6
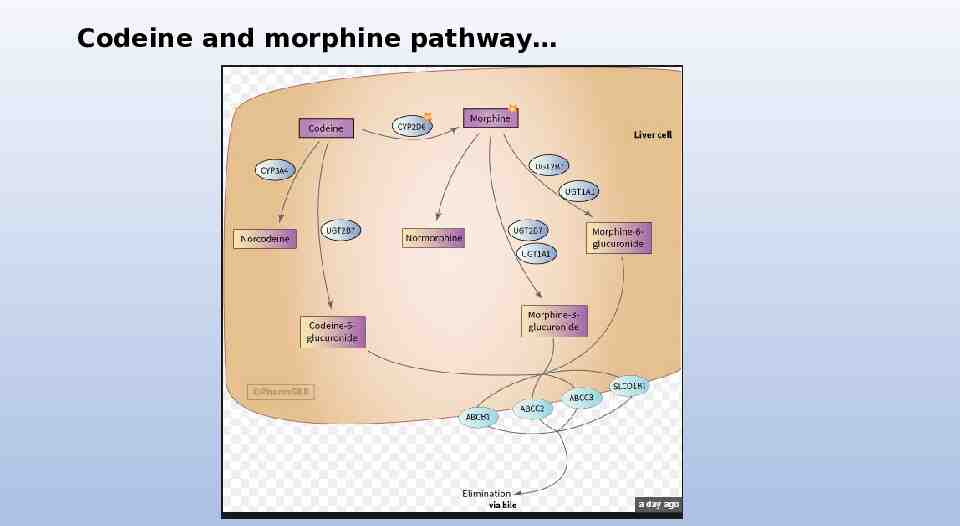
Codeine and morphine pathway
Main Opioid Compounds Encountered Clinically HYDROCODONE: Frequently prescribed for mild-to-moderate pain and is less potent and efficacious than is morphine. Often used co-formulated orally with acetaminophen (e.g., Vicodin, Lortab); thus, there can be hepatotoxicity associated with abuse of such formulations. OXYCODONE: Co-formulated for oral administration with aspirin (e.g., Percodan) or with acetaminophen (e.g., Percocet) for treatment of moderate pain. Also available in different formulations alone (e.g., Oxycontin). Has slightly lower efficacy than does morphine. Has become a frequent drug of abuse, especially in certain controlled release formulations, which can be crushed and selfadministered (intranasally or IV), for faster onset and bioavailability.
Main Opioid Compounds Encountered Clinically OXYMORPHONE: Prescribed for treatment of moderate-to-severe pain (e.g., Opana). Potent analgesic and has approximately equal efficacy to morphine. Frequent drug of abuse, especially in controlled release formulations, which can be crushed and self-administered. MEPERIDINE: Synthetic compound with similar efficacy to morphine. Prescription as an analgesic has been decreasing due to concerns of toxicity (e.g., proconvulsant effects, serotonin syndrome) of a major metabolite (normeperidine). Should not be used for 48 hours or at doses greater than 600 mg/day. Available orally and by injection. In some countries outside the United States (e.g., United Kingdom), meperidine is known as pethidine.
Main Opioid Compounds Encountered Clinically FENTANYL AND ITS ANALOGS: Synthetic and potent high-efficacy MOPr agonists. Used primarily by spinal/epidural or parenteral routes, in inpatient medical procedures. Fentanyl itself is also available by transdermal patch, for chronic severe pain. Fentanyl analogs are sometimes illicitly synthesized and abused and can be associated with great morbidity (respiratory depression), due to their potency, efficacy, and rapid onset. Fentanyl and its analogs are unique among the opioids in causing rapid chest wall rigidity refractory to mechanical ventilation unless naloxone or a neuromuscular blocking agent is administered.
Main Opioid Compounds Encountered Clinically PENTAZOCINE: Pentazocine (e.g., Talwin) is a “mixed agonist–antagonist” opioid (this category also includes nalbuphine and butorphanol). Such compounds have limited efficacy at MOPr (typically acting as partial agonists) and also partial KOPr agonist effects. Due to its low-efficacy actions at MOPr, pentazocine can cause withdrawal in patients dependent on MOPr agonists (e.g., Heroin). Due to its KOPr-mediated actions, pentazocine can produce dysphoria and psychotomimetic effects. Some oral formulations of pentazocine are co-formulated with naloxone, which is pharmacologically active only if the tablets are illicitly crushed and injected parenterally. Highly abused in the past but infrequently seen now among IV drug abusers. Often mixed with the antihistamine tripelennamine (T’s and Blues) as a potentiator, became popular in the 1980s due to the decline of the quality of street heroin. Severe side effects include seizures, pulmonary fibrosis, and soft tissue fibrosis at injections sites.
Main Opioid Compounds Encountered Clinically BUPRENORPHINE: Originally developed as an analgesic. MOPr partial agonist (and is also a KOPr partial agonist). Partial MOPr agonist effects of buprenorphine thus usually result in a maximum plateau to its effects (i.e., there is a lesser, but not absent, risk of overdose with this compound). Norbuprenorphine is an active buprenorphine metabolite in humans. Buprenorphine alone, a.k.a. buprenorphine monoproduct (e.g., Subutex), and in combination with naloxone (Suboxone), is approved (by the sublingual route) as an office-based treatment for heroin and opioid addiction. Addition of naloxone to the formulation is designed to minimize diversion and abuse, since naloxone could block buprenorphine effects, if this formulation were to be injected parenterally. Numerous reports of buprenorphine diversion and abuse, and clinically relevant respiratory depression can occur, especially if there is co-abuse with a benzodiazepine.
Main Opioid Compounds Encountered Clinically METHADONE: Synthetic long-acting full-efficacy MOPr agonist, active by oral and parenteral routes. Half-life of racemic methadone is approximately 24 hours, whereas its active l(r)-methadone enantiomer is approximately 48 hours. Used primarily as a daily oral maintenance treatment for heroin addiction since initial studies in 1964 and was approved by the FDA in 1972. Also effective in the treatment of chronic pain. Should not be used in opioid-naïve patients, due to the risk of respiratory depression due to the initial metabolic accumulation of daily methadone, which could lead to overdose in opioid-naïve patients. Methadone is available as a racemate in the united states (and most other countries).
METHADONE: MOPr agonist activity and thus most of its effects are primarily caused by the l(r)-methadone enantiomer. Both methadone enantiomers are weak NMDA antagonists, and this adjunctive action may be beneficial, in decreasing the progression of tolerance during chronic dosing. Patients in methadone maintenance can remain at individually determined effective doses for prolonged periods, with limited need for escalation. Long-term maintenance with sufficient doses of methadone (in most cases 80 to 150 mg/day) has a beneficial effect on health status, resulting in decreased relapse and decreased risk of acquisition of new infectious diseases. Methadone maintenance programs (as well as buprenorphine–naloxone maintenance programs) should be supplemented by appropriate psychosocial and medical support, to further help recovery in all spheres of patient life.
Opioid Antagonists NALOXONE (e.g., Narcan): Short-acting injectable antagonist, is used primarily for reversal of MOPr agonist overdose (e.g., due to heroin or prescription opioids). Duration of action is in the 30 to 60 minutes range; therefore, if overdose with a longer-acting opioid is suspected, patients should be monitored and repeat naloxone administration or infusion may be necessary. Low oral bioavailability and therefore must be administered by other routes. Doses typically used for overdose reversal are in the range 0.4 to 2 mg (IV, IM, or SC; several states and jurisdictions have also allowed intranasal administration). Doses 2 mg are often used now because of the recent upswing in the use of fentanyl. Dosage can be repeated every 2 to 3 minutes to effect (e.g., reversal of respiratory depression), not to exceed 10 mg. In patients with suspected opioid dependence (e.g., due to history of chronic use), the emergence of withdrawal symptoms should be expected and managed following naloxone administration.
Opioid Antagonists NALTREXONE: is Available orally for the treatment of alcoholism and OUD (e.g., used daily) or as a monthly depot injection (Vivitrol) the treatment of alcoholism or prevention of relapse to opioid misuse. NALMEFENE: Recently approved in the United States for reversal of MOPr agonist effects by parenteral routes. Has a longer duration of action than naloxone and has greater oral bioavailability. Recently approved in certain European countries as an oral formulation, for the treatment of alcoholism.
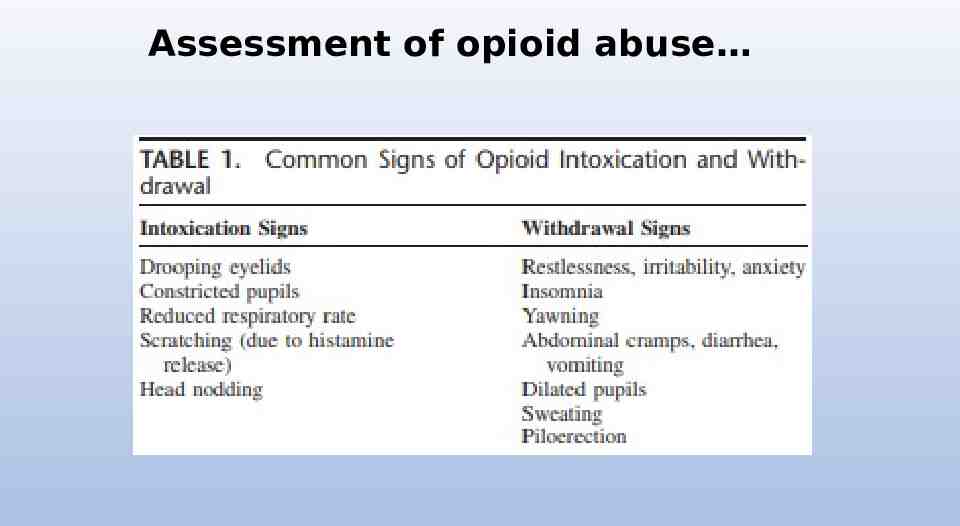
Assessment of opioid abuse
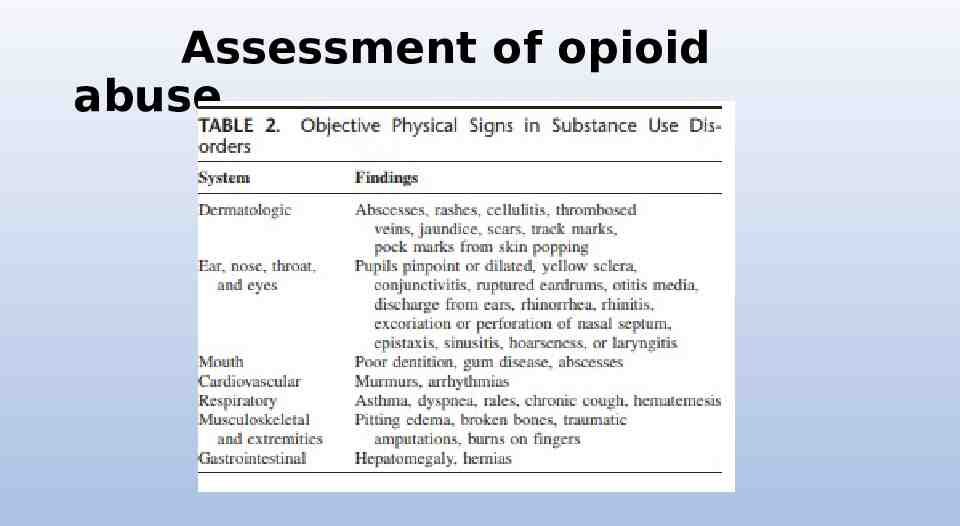
Assessment of opioid abuse
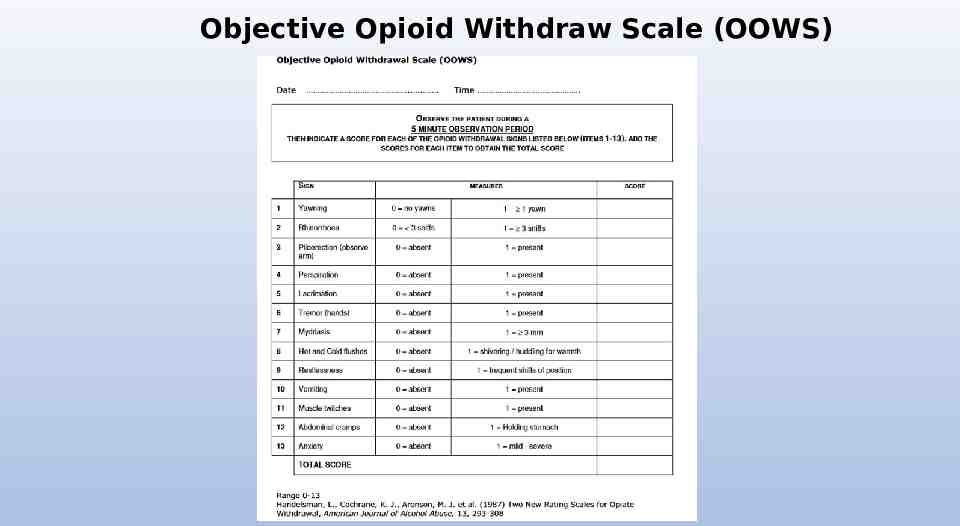
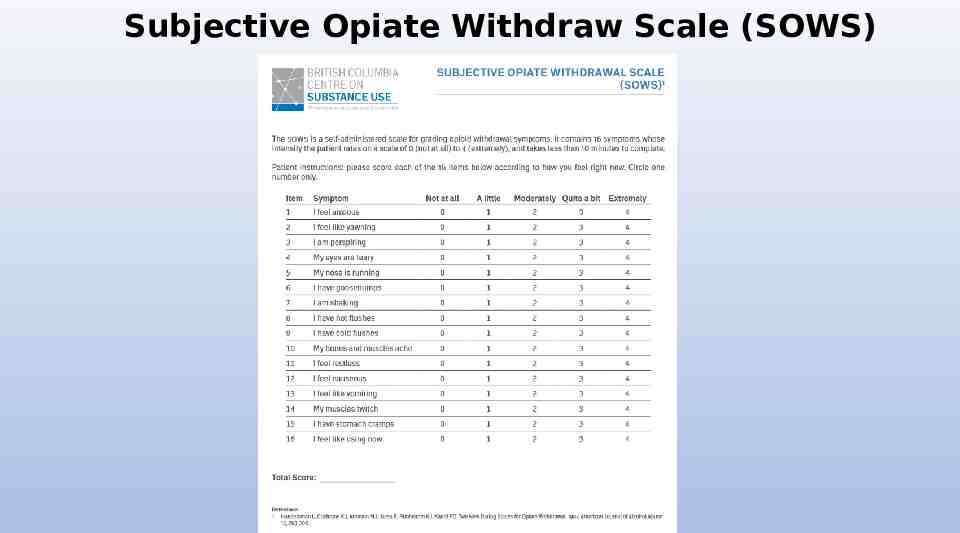
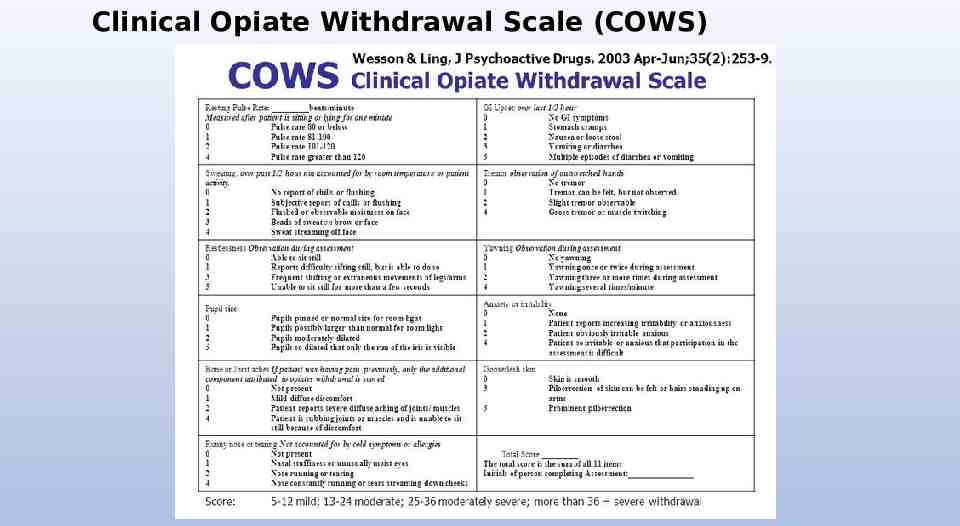
Assessment of Opioid Withdrawal Validated clinical scales that measure withdrawal symptoms may be used to assist in the evaluation of patients with opioid use disorder (OUD): Examples include: The Objective Opioid Withdrawal Scale (00WS) The Subjective Opioid Withdrawal Scale (S0WS) The Clinical Opioid Withdraw Scale (COWS)
Objective Opioid Withdraw Scale (OOWS)
Subjective Opiate Withdraw Scale (SOWS)
Clinical Opiate Withdrawal Scale (COWS)
Treatment of opioid withdrawal: General Principles Choice of available treatment options should be a shared decision between clinician and patient. Clinicians should consider the patient’s preferences, past treatment history, and treatment setting when deciding between the use of methadone, buprenorphine, and naltrexone in the treatment of addiction involving opioid use. The venue in which treatment is provided is as important as the specific medication selected. Using medications for opioid withdrawal management is recommended over abrupt cessation of opioids for most patients.
Treatment of opioid withdrawal: General Principles Patients should be advised about risk of relapse and other safety concerns from using opioid withdrawal management as stand-alone treatment for OUD. Assessment of a patient undergoing opioid withdrawal management should include a thorough medical history and physical examination focusing on signs and symptoms associated with opioid withdrawal. 2 primary types of MAT treatment for opioid withdrawal are: Office-Based Opioid Treatment (OBOT) buprenorphine Opioid Treatment Programs (OTP) methadone
Treatment of opioid withdrawal: General Principles OBOT may not be suitable for patients with active alcohol use disorder or sedative-hypnotic, or anxiolytic use disorder. Methadone is recommended for patients who may benefit from daily dosing and supervision in an OTP or for patients for whom buprenorphine for the treatment of OUD has been used unsuccessfully in an OTP or OBOT setting. Oral naltrexone for the treatment of an OUD is often adversely affected by poor medication adherence. Opioid withdrawal management in cases in which buprenorphine is used to manage withdrawal symptoms should not be initiated until: 12-18 hours after the last dose of a short-acting agonist such as heroin or oxycodone. 24-48 hours after the last dose of a long-acting agonist such as methadone. Opioid withdrawal management using anesthesia ultra-rapid opioid detoxification (UROD) is NOT recommended due to high risk for adverse events or death. The use of combinations of buprenorphine and low doses of oral naltrexone to manage withdrawal and facilitate the accelerated introduction of extendedrelease injectable naltrexone has shown promise but is still in the study phase.
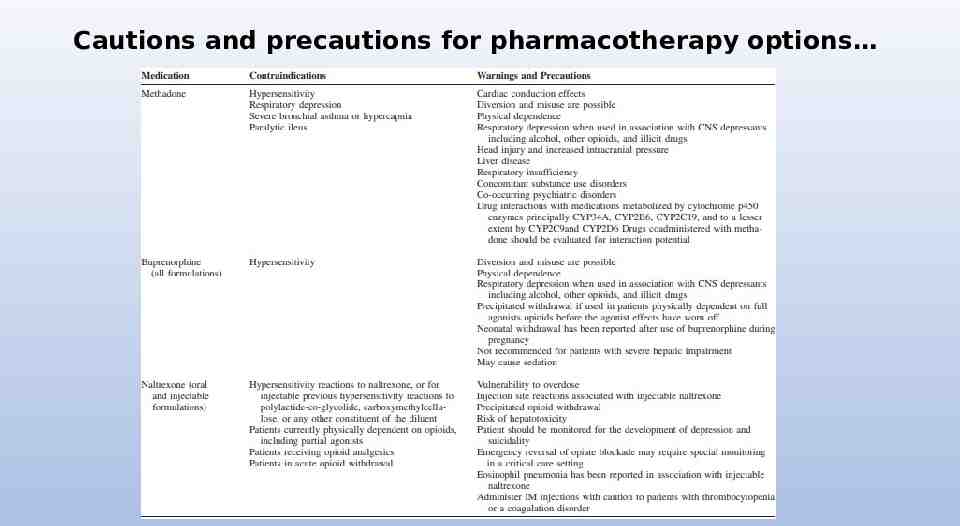
Cautions and precautions for pharmacotherapy options
Methadone Treatment option recommended for patients who are physiologically dependent on opioids, able to give informed consent, and who have no specific contraindications for agonist treatment when it is prescribed in the context of an appropriate plan that includes psychosocial intervention. Recommended initial dose ranges for methadone are from 10-30 mg with reassessment in 3-4 hours, and a 2nd dose not to exceed 10 mg on the first day if withdrawal symptoms are persisting. Usual daily dose of methadone ranges from 60-120 mg. Dosage increases in 5-10 mg increments applied no more frequently than every 7 days (depending on the clinical response) are necessary to avoid over-sedation, toxicity, or even iatrogenic overdose deaths.
Methadone OTP regulations require monitored medication administration until the patient’s clinical response and behavior demonstrates the prescribing of non—monitored doses is appropriate. Psychosocial treatment should be implemented in conjunction with the use of methadone in the treatment of OUD. Methadone should be reinstituted immediately if relapse occurs, or when an assessment determines that the risk of relapse as high. Relapse prevention strategies are a key component to OTP. Switching from methadone to another MAT medication may be appropriate if the patient experiences intolerable side effects or is not successful in attaining or maintaining treatment goals with methadone.
Methadone Patients switching from methadone to buprenorphine in the treatment of OUD should be on low doses of methadone prior to switching medications: Patients on 30-40 mg of methadone per day or less generally tolerate transition to buprenorphine with minimal discomfort Patients switching from methadone to oral naltrexone or extended-release injectable naltrexone (Vivitrol) must be completely withdrawn from methadone and other opioids before they can receive naltrexone. Patients who discontinue agonist therapy with methadone or buprenorphine and then resume opioid use be made aware of the risks associated with opioid overdose, and especially the increased risk of death.
Buprenorphine Opioid-dependent patients should wait until they are experiencing mild to moderate opioid withdrawal (COWS score of 8-12) before taking the first dose of buprenorphine to reduce the risk of precipitated withdrawal: Generally, buprenorphine initiation should occur at least 6-12 hours after the last use of heroin or other short-acting opioids, or 24-72 hours after the last use of long acting opioids such as methadone. Induction of buprenorphine should start with a dose of 2-4 mg and dosages may be increased in increments of 2-4 mg: Maximum first day dose should not exceed 8 mg.
Buprenorphine Clinicians should observe patients and their offices during induction. (However, home buprenorphine induction may be considered) Buprenorphine doses after induction and titration should be, on average, 8 mg per day: If patients are continuing to use opioids, consideration should be given to increasing the dose by 4-8 mg (daily doses of 12-16 mg or higher). FDA approves dosing to a limit of 24 mg per day and there is limited evidence regarding the relative efficacy of higher doses.
Buprenorphine Psychosocial treatment should be implemented in conjunction with the use of buprenorphine in the treatment of OUD. To reduce the chances of diversion of buprenorphine clinicians should: Include frequent office visits (weekly in early treatment). Urine drug testing which includes buprenorphine and its metabolites Recall visits for pill counts Access Prescription Drug Monitoring Program (KASPER) data frequently.
Buprenorphine Buprenorphine taper and discontinuation is a slow process and close monitoring is recommended: This is generally accomplished over several months. Patient should be encouraged to remain in treatment for ongoing monitoring past the point of discontinuation. Allow 7-14 days between last dose of buprenorphine and initiation of naltrexone to avoid precipitating withdrawal. When switching from buprenorphine to methadone there is no required time delay since the addition of a full mu opioid agonist to a partial agonist does not typically result in any type of adverse reaction If patients choose to self-discontinue their buprenorphine they must be reminded of the dangers of relapse and overdose.
Naltrexone Naltrexone is a recommended treatment in preventing relapse in OUD. Oral naltrexone may be considered for patients where adherence can be supervised or enforced. Extended-release injectable naltrexone (Vivitrol) may be more suitable for patients who have issues with adherence. Oral naltrexone should be taken daily in 50 mg doses, or three times weekly in 100 mg doses followed by one 150 mg dose. Vivitrol should be administered Q4 weeks by deep IM in the gluteal muscle at a set dosage of 380 mg per injection. Psychosocial treatment is recommended in conjunction with treatment with naltrexone
Naltrexone There is no recommended length of treatment with oral naltrexone or Vivitrol. Duration depends on clinical judgment and the patient’s individual circumstances. Because there is no physical dependence associated with naltrexone, it can be stopped abruptly without withdrawal symptoms. Switching from naltrexone to methadone or buprenorphine should be planned, considered, and monitored. Switching from an antagonist (naltrexone) to a partial agonist (buprenorphine) or a full agonist (methadone) is less complicated than switching in the opposite direction. Patient is being switched from naltrexone to be for an orphan or methadone will not have physical dependence on opioids and thus the initial doses of either medication used should be low.
Psychosocial treatment in conjunction with medications for the treatment of OUD Psychosocial treatment is recommended in conjunction with any pharmacological treatment of OUD. Treatment planning should include collaboration with qualified behavioral healthcare providers determine the optimal type and intensity of psychosocial treatment. Psychosocial treatment should be offered with any of the aforementioned medications used in treating OUD
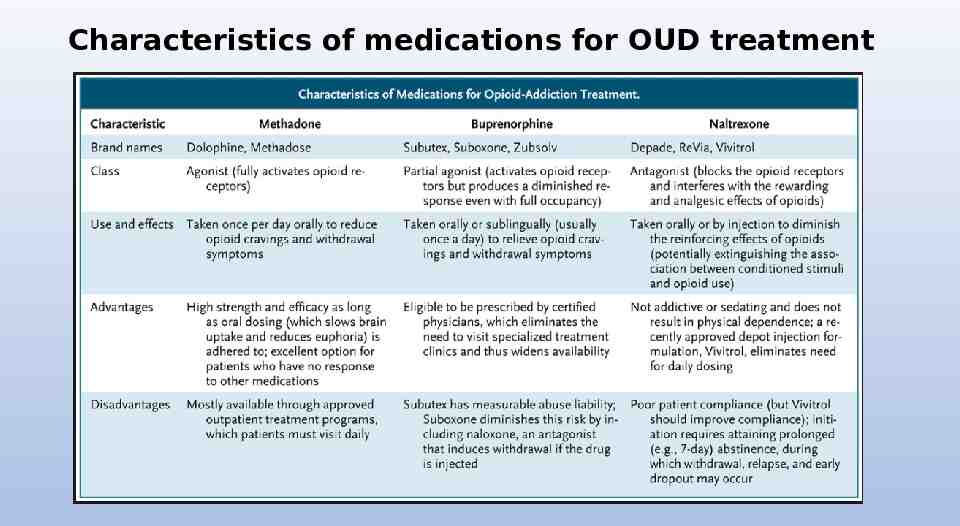
Characteristics of medications for OUD treatment
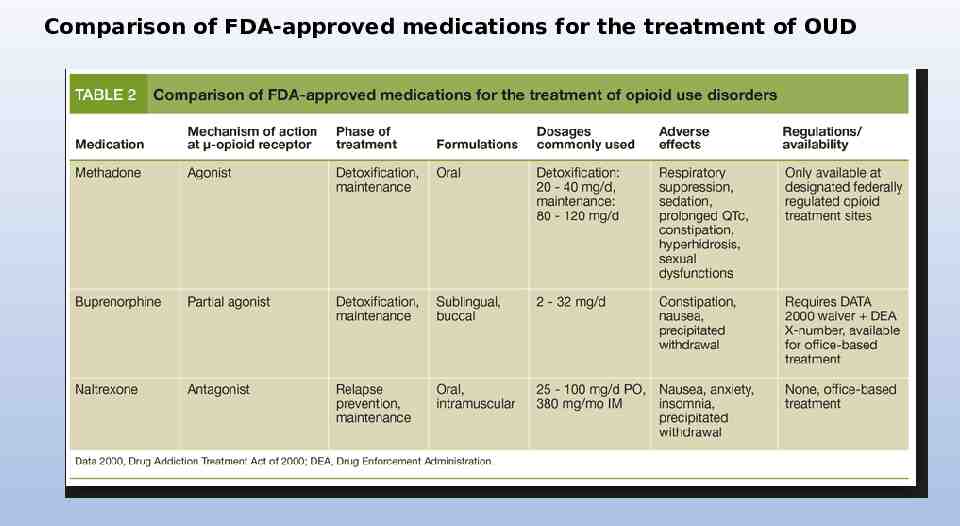
Comparison of FDA-approved medications for the treatment of OUD
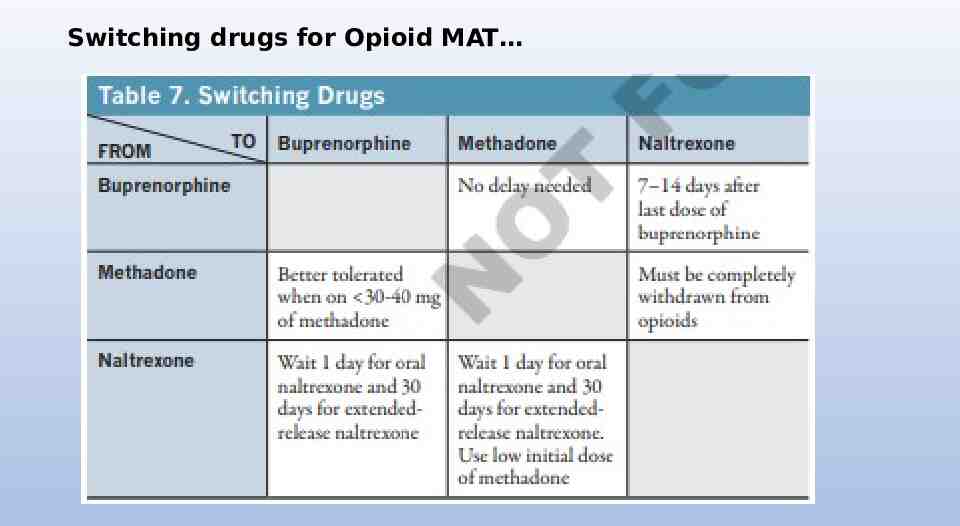
Switching drugs for Opioid MAT
Special Populations: Pregnant Women First priority in evaluating pregnant women for OUD is to identify emergent or urgent medical conditions that require immediate referral for clinical evaluation. Medical examination and psychosocial assessment is highly recommended. Counseling and testing for HIV should be provided in accordance with state law. Test for hepatitis A, B, and C and liver functions are also suggested. Urine drug testing may be used to detect or confirm suspected opioid and other drug use with informed consent from the mother, realizing that there may be adverse legal and social consequences of her use. Pregnant women who are physically dependent on opioids should receive treatment using methadone or buprenorphine monoproduct (e.g., Subutex) rather than withdrawal management or abstinence.
Special Populations: Pregnant Women Treatment with methadone should be initiated as early as possible during pregnancy: Hospitalization during initiation of methadone in treatment with buprenorphine may be advisable due to the potential for adverse events, especially in the third trimester. In an inpatient setting, methadone should be initiated at a dose range of 20-30 mg. Incremental doses of 5-10 mg are given every 3 to 6 hours as needed to treat withdrawal symptoms. After induction, clinicians should increase the methadone dose and 5-10 mg increments per week.
Special Populations: Pregnant Women The goal is to maintain the lowest dose the controls withdrawal symptoms and minimizes craving. Twice daily dosing is more effective and has fewer side effects than single dosing but may not be practical because methadone is typically dispensed in an outpatient clinic. Care for pregnant women with OUD should be co-managed by an obstetrician and addiction specialist physician. Clinicians should be aware that the pharmacokinetics of methadone are affected by pregnancy: With advancing gestational age, plasma level levels of methadone progressively decrease and clearance increases. Increased or split doses may be needed as pregnancy progresses After delivery doses may need to be adjusted
Special Populations: Pregnant Women Buprenorphine monoproduct (Subutex) is a reasonable and recommended alternative to methadone for pregnant women. While there is evidence of safety, there is insufficient evidence to recommend the combination buprenorphine/naloxone formulation (e.g., Suboxone). If a woman becomes pregnant while receiving naltrexone, is appropriate to discontinue the medication if the patient and doctor agree that the risk of relapse is low. If the patient wishes to discontinue naltrexone but then reports relapsed opioid use it may be appropriate to consider treatment with methadone or buprenorphine.
Special Populations: Pregnant Women Naloxone is NOT recommended for use in pregnant women with OUD except in situations of life-threatening overdose. Mother is receiving methadone and buprenorphine monitor product for the treatment of OUDs SHOULD be encouraged to breast-feed.
Special Populations: Patients with Pain For all patients with pain, it is important that the correct diagnosis be made and that a target suitable for treatment is identified. If pharmacological treatment is considered, nonnarcotic medications such as acetaminophen and NSAIDs should be tried first. Opioid agonists (methadone or buprenorphine) should be considered for patients with active OUD who are not in treatment. Pharmacotherapy in conjunction with psychosocial treatment should be considered for patients with pain who have OUD.
Special Populations: Patients with Pain Patients on methadone maintenance will require doses of opioids in addition to their regular daily dose of methadone to manage acute pain. Patient is on methadone maintenance who are admitted for surgery may require additional short-acting opioid pain relievers. Temporarily increasing buprenorphine dosing may be effective for mild acute pain. For severe acute pain, discontinuing buprenorphine and commencing on a high potency opioid (such as Fentanyl) is advisable.
Special Populations: Patients with Pain The decision to discontinue buprenorphine prior to an elective surgical procedure should be made in consultation with the attending surgeon and anesthesiologist. If it is decided that buprenorphine should be discontinued prior to surgery, this should occur 24-36 hours in advance of surgery and restart it postoperatively when the need for full opioid agonist analgesia has passed.
Special Populations: Patients with Pain PATIENTS ON NALTREXONE WILL NOT RESPOND TO OPIOID ANALGESICS IN THE USUAL MANNER: Mild pain may be treated with NSAIDs. moderate to severe pain may be treated with ketorolac on a short-term basis studies are currently underway at looking at the use of low-dose ketamine for the treatment of pain in patients on naltrexone Oral naltrexone should be discontinued 72 hours prior to elective surgery and extended-release injectable naltrexone (Vivitrol) should be discontinued 30 days prior to an anticipated surgery.
Special Populations: Adolescents Clinician should consider treating adolescents who have OUD using the full range of treatment options, including pharmacotherapy. Methadone, buprenorphine, and naltrexone may all be considered for treatment of OUD in adolescents. Age is a consideration in treatment and federal laws and FDA approvals need to be considered for patients under age 18. Psychosocial treatment is recommended Adolescents may benefit from treatment and specialized treatment facilities that provide multidimensional services.
Special Populations: Co-occurring psychiatric disorders Comprehensive assessment including determination of mental health status should evaluate whether the patient is stable. Suicide risk assessment is a must! Assessment for psychiatric disorders should occur at the onset of agonist or antagonist treatment: Reassessment using a detailed mental status examination should occur after stabilization with methadone, buprenorphine or naltrexone
Special Populations: Individuals in the Criminal Justice System Opioid MAT has been shown to be effective and is recommended by some addiction specialists for prisoners and parolees regardless of the length of the sentence time. This is a highly controversial issue Methadone, buprenorphine, or naltrexone may all be considered for maintenance. Pharmacotherapy should be initiated a minimum of 30 days prior to release from prison.
What about benzos “FDA Drug Safety Communication: FDA urges caution about withholding opioid addiction medications from patients taking benzodiazepines or CNS depressants: careful medication management can reduce risks.” Announcement [9-20-2017] FDA Safety Should generally restrict to low-dose short term use You need to know your patient!!
Questions or comments?