Mosunetuzumab Monotherapy Continues to Demonstrate Durable

16 Slides301.09 KB
Mosunetuzumab Monotherapy Continues to Demonstrate Durable Responses in Patients with Relapsed and/or Refractory Follicular Lymphoma after 2 Prior Therapies: 3-Year Follow-Up from a Pivotal Phase II Study Stephen J. Schuster,1 Laurie H. Sehn,2 Nancy L. Bartlett,3 Matthew Matasar,4 Sarit Assouline,5 Pratyush Giri,6 John Kuruvilla,7 Mazyar Shadman,8 Chan Y. Cheah,9 Sascha Dietrich,10 Keith Fay,11 Matthew Ku,12 Loretta Nastoupil,13 Michael C. Wei,14 Shen Yin,14 Iris To,14 Samuel Tracy,14 Antonia Kwan,14 Elicia Penuel,14 L. Elizabeth Budde15 Lymphoma Program, Abramson Cancer Center, University of Pennsylvania, Philadelphia, PA, USA; 2BC Cancer Centre for Lymphoid Cancer and The University of British Columbia, Vancouver, BC, Canada; 3Siteman Cancer Center, Washington University School of Medicine, St. Louis, MO, USA; 4Rutgers Cancer Institute of New Jersey, New Brunswick, NJ, USA; 5Jewish General Hospital, Montreal, QC, Canada; 6Royal Adelaide Hospital, Adelaide, Australia; 7Princess Margaret Cancer Centre, Toronto, ON, Canada; 8Fred Hutchinson Cancer Research Center and University of Washington, Seattle, WA, USA; 9Linear Clinical Research, Sir Charles Gairdner Hospital, Nedlands, Australia and The University of Western Australia, Perth, Australia; 10Universitat Heidelberg, Heidelberg, Germany; 11St Vincent's Hospital and Royal North Shore Hospital, Sydney, Australia; 12St Vincent's Hospital, University of Melbourne, Melbourne, Australia; 13MD Anderson Cancer Center, Houston, TX, USA; 14 Genentech, Inc., South San Francisco, CA, USA; 15City of Hope National Medical Center, Duarte, CA, USA Presented at the 65th ASH Annual Meeting December 9–12, 2023 M-DE-00019686 1
Disclaimer: Lunsumio (Mosunetuzumab) Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 Dieses Arzneimittel unterliegt einer zusätzlichen Überwachung. Dies ermöglicht eine schnelle Identifizierung neuer Erkenntnisse über die Sicherheit. Angehörige von Gesundheitsberufen sind aufgefordert, jeden Verdachtsfall einer Nebenwirkung zu melden. Bitte melden Sie Nebenwirkungen an die Roche Pharma AG unter grenzach.drug [email protected] oder Fax 49 7624/14-3183 oder an das Paul-Ehrlich-Institut unter www.pei.de oder Fax: 49 6103/77-1234.
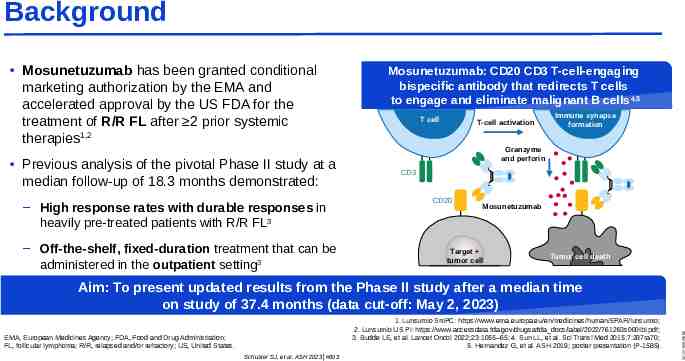
Background Mosunetuzumab has been granted conditional marketing authorization by the EMA and accelerated approval by the US FDA for the treatment of R/R FL after 2 prior systemic therapies1,2 Previous analysis of the pivotal Phase II study at a median follow-up of 18.3 months demonstrated: – High response rates with durable responses in heavily pre-treated patients with R/R FL3 – Off-the-shelf, fixed-duration treatment that can be administered in the outpatient setting3 Mosunetuzumab: CD20 CD3 T-cell-engaging bispecific antibody that redirects T cells to engage and eliminate malignant B cells 4,5 T cell T-cell activation Immune synapse formation Granzyme and perforin CD3 CD20 Mosunetuzumab Target tumor cell Tumor cell death 1. Lunsumio SmPC: https://www.ema.europa.eu/en/medicines/human/EPAR/lunsumio; 2. Lunsumio US PI: https://www.accessdata.fda.gov/drugsatfda docs/label/2022/761263s000lbl.pdf; 3. Budde LE, et al. Lancet Oncol 2022;23:1055–65; 4. Sun LL, et al. Sci Transl Med 2015;7:287ra70; 5. Hernandez G, et al. ASH 2019; poster presentation (P-1585). EMA, European Medicines Agency; FDA, Food and Drug Administration; FL, follicular lymphoma; R/R, relapsed and/or refractory; US, United States. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 Aim: To present updated results from the Phase II study after a median time on study of 37.4 months (data cut-off: May 2, 2023)
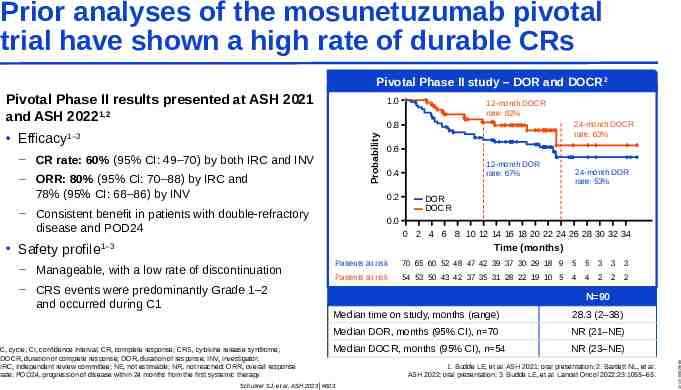
Prior analyses of the mosunetuzumab pivotal trial have shown a high rate of durable CRs Pivotal Phase II study – DOR and DOCR 2 Pivotal Phase II results presented at ASH 2021 and ASH 20221,2 – CR rate: 60% (95% CI: 49‒70) by both IRC and INV – ORR: 80% (95% CI: 70‒88) by IRC and 78% (95% CI: 68‒86) by INV 24-month DOCR rate: 63% 0.6 12-month DOR rate: 67% 0.4 0.2 – Consistent benefit in patients with double-refractory disease and POD24 24-month DOR rate: 53% DOR DOCR 0.0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 Time (months) 1‒3 – Manageable, with a low rate of discontinuation – CRS events were predominantly Grade 1–2 and occurred during C1 C, cycle; CI, confidence interval; CR, complete response; CRS, cytokine release syndrome; DOCR, duration of complete response; DOR, duration of response; INV, investigator; IRC, independent review committee; NE, not estimable; NR, not reached; ORR, overall response rate; POD24, progression of disease within 24 months from the first systemic therapy. Patients at risk 70 65 60 52 48 47 42 39 37 30 29 18 9 5 5 3 3 3 Patients at risk 54 53 50 43 42 37 35 31 28 22 19 10 5 4 4 2 2 2 N 90 Median time on study, months (range) 28.3 (2–38) Median DOR, months (95% CI), n 70 NR (21–NE) Median DOCR, months (95% CI), n 54 NR (23–NE) Schuster SJ, et al. ASH 2023 #603 1. Budde LE, et al. ASH 2021; oral presentation; 2. Bartlett NL, et al. ASH 2022; oral presentation; 3. Budde LE, et al. Lancet Oncol 2022;23:1055–65. M-DE-00019686 Safety profile 12-month DOCR rate: 82% 0.8 1‒3 Probability Efficacy 1.0
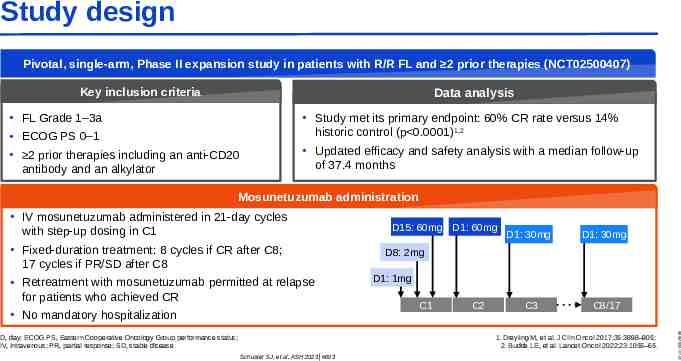
Study design Pivotal, single-arm, Phase II expansion study in patients with R/R FL and 2 prior therapies (NCT02500407) Key inclusion criteria Data analysis FL Grade 1–3a ECOG PS 0–1 2 prior therapies including an anti-CD20 antibody and an alkylator Study met its primary endpoint: 60% CR rate versus 14% historic control (p 0.0001)1,2 Updated efficacy and safety analysis with a median follow-up of 37.4 months Mosunetuzumab administration D, day; ECOG PS, Eastern Cooperative Oncology Group performance status; IV, intravenous; PR, partial response; SD, stable disease. D15: 60mg D1: 60mg D1: 30mg D1: 30mg C3 C8/17 D8: 2mg D1: 1mg C1 C2 1. Dreyling M, et al. J Clin Oncol 2017;35:3898–905; 2. Budde LE, et al. Lancet Oncol 2022;23:1055–65. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 IV mosunetuzumab administered in 21-day cycles with step-up dosing in C1 Fixed-duration treatment: 8 cycles if CR after C8; 17 cycles if PR/SD after C8 Retreatment with mosunetuzumab permitted at relapse for patients who achieved CR No mandatory hospitalization
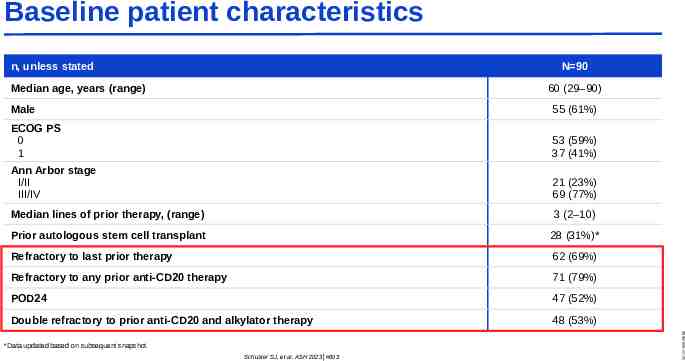
Baseline patient characteristics n, unless stated N 90 60 (29–90) Male 55 (61%) ECOG PS 0 1 53 (59%) 37 (41%) Ann Arbor stage I/II III/IV 21 (23%) 69 (77%) Median lines of prior therapy, (range) 3 (2–10) Prior autologous stem cell transplant 28 (31%)* Refractory to last prior therapy 62 (69%) Refractory to any prior anti-CD20 therapy 71 (79%) POD24 47 (52%) Double refractory to prior anti-CD20 and alkylator therapy 48 (53%) *Data updated based on subsequent snapshot. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 Median age, years (range)
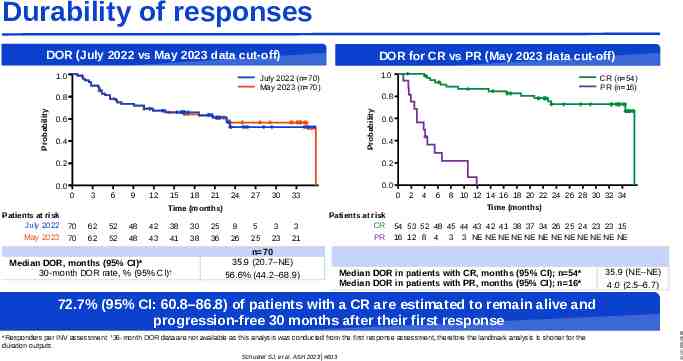
Durability of responses DOR (July 2022 vs May 2023 data cut-off) 1.0 DOR for CR vs PR (May 2023 data cut-off) 1.0 July 2022 (n 70) May 2023 (n 70) 0.8 Probability Probability 0.8 0.6 0.4 0.4 0.0 0.0 0 May 2023 0.6 0.2 0.2 Patients at risk July 2022 CR (n 54) PR (n 16) 3 6 9 12 15 18 21 24 27 30 Time (months) 70 70 62 62 52 52 48 48 42 43 38 41 Median DOR, months (95% CI)* 30-month DOR rate, % (95% CI)† 30 38 25 36 9 26 5 25 3 23 0 33 3 21 Patients at risk CR n 70 35.9 (20.7–NE) 56.6% (44.2–68.9) PR 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 Time (months) 54 53 52 48 45 44 43 42 41 38 37 34 26 25 24 23 23 15 16 12 8 4 3 3 NE NE NE NE NE NE NE NE NE NE NE NE Median DOR in patients with CR, months (95% CI); n 54* Median DOR in patients with PR, months (95% CI); n 16* 35.9 (NE–NE) 4.0 (2.5–6.7) *Responders per INV assessment. †36-month DOR data are not available as this analysis was conducted from the first response assessment, therefore the landmark analysis is shorter for the duration outputs. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 72.7% (95% CI: 60.8–86.8) of patients with a CR are estimated to remain alive and progression-free 30 months after their first response
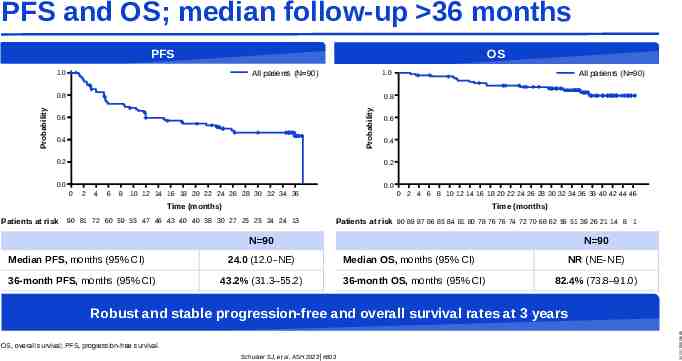
PFS and OS; median follow-up 36 months PFS OS All patients (N 90) 1.0 1.0 0.8 Probability Probability 0.8 All patients (N 90) 0.6 0.4 0.2 0.6 0.4 0.2 0.0 0.0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 Time (months) Patients at risk Time (months) 90 81 72 60 59 55 47 46 43 40 40 38 30 27 25 25 24 24 13 Patients at risk 90 89 87 86 85 84 81 80 78 76 76 74 72 70 68 62 56 51 39 26 21 14 8 1 N 90 Median PFS, months (95% CI) 36-month PFS, months (95% CI) 24.0 (12.0–NE) 43.2% (31.3–55.2) N 90 Median OS, months (95% CI) 36-month OS, months (95% CI) NR (NE–NE) 82.4% (73.8–91.0) OS, overall survival; PFS, progression-free survival. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 Robust and stable progression-free and overall survival rates at 3 years
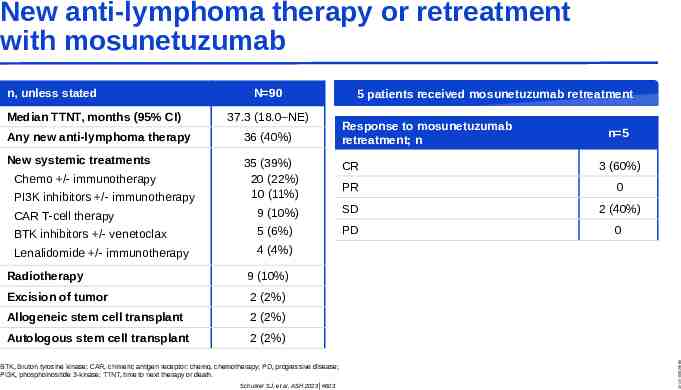
New anti-lymphoma therapy or retreatment with mosunetuzumab Median TTNT, months (95% CI) N 90 37.3 (18.0–NE) 5 patients received mosunetuzumab retreatment Response to mosunetuzumab retreatment; n n 5 Any new anti-lymphoma therapy 36 (40%) New systemic treatments 35 (39%) 20 (22%) 10 (11%) CR 3 (60%) PR 0 CAR T-cell therapy 9 (10%) SD 2 (40%) BTK inhibitors /- venetoclax 5 (6%) PD 0 Lenalidomide /- immunotherapy 4 (4%) Chemo /- immunotherapy PI3K inhibitors /- immunotherapy Radiotherapy 9 (10%) Excision of tumor 2 (2%) Allogeneic stem cell transplant 2 (2%) Autologous stem cell transplant 2 (2%) BTK, Bruton tyrosine kinase; CAR, chimeric antigen receptor; chemo, chemotherapy; PD, progressive disease; PI3K, phosphoinositide 3-kinase; TTNT, time to next therapy or death. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 n, unless stated
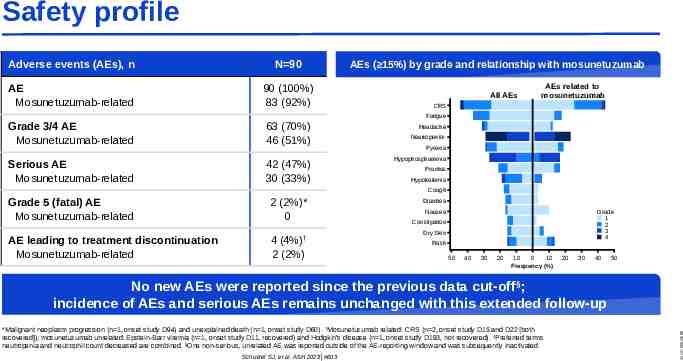
Safety profile Adverse events (AEs), n N 90 AE Mosunetuzumab-related 90 (100%) 83 (92%) AEs ( 15%) by grade and relationship with mosunetuzumab All AEs AEs related to mosunetuzumab CRS Fatigue Grade 3/4 AE Mosunetuzumab-related 63 (70%) 46 (51%) Serious AE Mosunetuzumab-related 42 (47%) 30 (33%) Grade 5 (fatal) AE Mosunetuzumab-related 2 (2%)* 0 AE leading to treatment discontinuation Mosunetuzumab-related 4 (4%)† 2 (2%) Headache Neutropenia‡ Pyrexia Hypophosphatemia Pruritus Hypokalemia Cough Diarrhea Nausea Grade 1 2 3 4 Constipation Dry Skin Rash 50 40 30 20 10 0 10 Frequency (%) 20 30 40 50 *Malignant neoplasm progression (n 1, onset study D94) and unexplained death (n 1, onset study D60). †Mosunetuzumab related: CRS (n 2, onset study D15 and D22 [both recovered]); mosunetuzumab unrelated: Epstein-Barr viremia (n 1, onset study D11, recovered) and Hodgkin’s disease (n 1, onset study D193, not recovered). ‡Preferred terms neutropenia and neutrophil count decreased are combined. §One non-serious, unrelated AE was reported outside of the AE-reporting window and was subsequently inactivated. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 No new AEs were reported since the previous data cut-off§; incidence of AEs and serious AEs remains unchanged with this extended follow-up
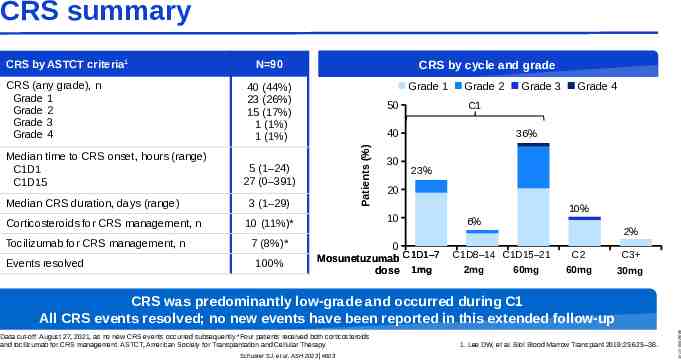
CRS summary CRS (any grade), n Grade 1 Grade 2 Grade 3 Grade 4 Median time to CRS onset, hours (range) C1D1 C1D15 Median CRS duration, days (range) Corticosteroids for CRS management, n Tocilizumab for CRS management, n Events resolved N 90 CRS by cycle and grade Grade 1 40 (44%) 23 (26%) 15 (17%) 1 (1%) 1 (1%) 50 5 (1–24) 27 (0–391) 3 (1–29) 100% 30 Grade 3 Grade 4 C1 36% 23% 20 10 10 (11%)* 7 (8%)* Grade 2 40 Patients (%) CRS by ASTCT criteria1 0 Mosunetuzumab C1D1–7 dose 1mg 10% 6% 2% C1D8–14 C1D15–21 2mg 60mg C2 C3 60mg 30mg Data cut-off: August 27, 2021, as no new CRS events occurred subsequently.*Four patients received both corticosteroids and tocilizumab for CRS management. ASTCT, American Society for Transplantation and Cellular Therapy. Schuster SJ, et al. ASH 2023 #603 1. Lee DW, et al. Biol Blood Marrow Transplant 2019;25:625–38. M-DE-00019686 CRS was predominantly low-grade and occurred during C1 All CRS events resolved; no new events have been reported in this extended follow-up
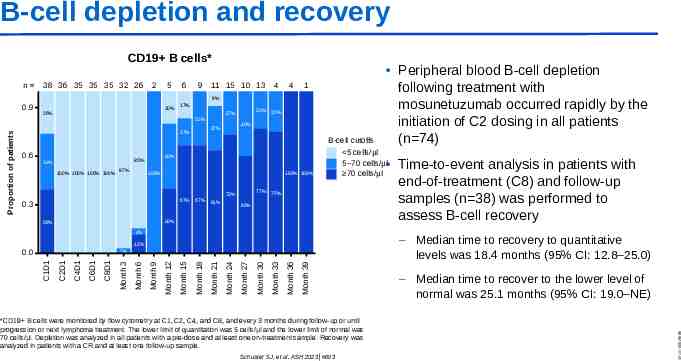
B-cell depletion and recovery CD19 B cells* 38 36 35 35 35 32 26 2 5 6 9 11 15 10 13 4 4 1 9% 0.9 20% 26% 17% Proportion of patients 0.6 40% 85% 34% 100% 100% 100% 100% 97% 25% 40% 27% 17% 23% 27% 33% 100% 100% 100% 67% 0.3 67% 77% 73% 64% B-cell cutoffs 5 cells/µl 5 70 cells/µl 70 cells/µl 75% 60% 40% 39% 4% 12% 0.0 Month 39 Month 36 Month 33 Month 30 Month 27 Month 24 Month 21 Month 18 Month 15 Month 12 Month 9 Month 6 Month 3 C8D1 C6D1 C4D1 C2D1 C1D1 3% *CD19 B cells were monitored by flow cytometry at C1, C2, C4, and C8, and every 3 months during follow-up or until progression or next lymphoma treatment. The lower limit of quantitation was 5 cells/μl and the lower limit of normal was 70 cells/μl. Depletion was analyzed in all patients with a pre-dose and at least one on-treatment sample. Recovery was analyzed in patients with a CR and at least one follow-up sample. Schuster SJ, et al. ASH 2023 #603 Time-to-event analysis in patients with end-of-treatment (C8) and follow-up samples (n 38) was performed to assess B-cell recovery – Median time to recovery to quantitative levels was 18.4 months (95% CI: 12.8–25.0) – Median time to recover to the lower level of normal was 25.1 months (95% CI: 19.0–NE) M-DE-00019686 n Peripheral blood B-cell depletion following treatment with mosunetuzumab occurred rapidly by the initiation of C2 dosing in all patients (n 74)
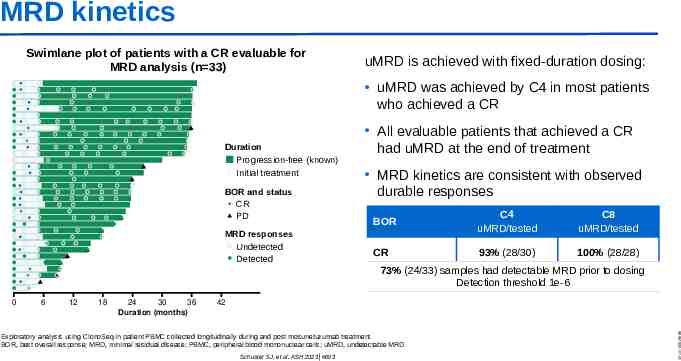
MRD kinetics Swimlane plot of patients with a CR evaluable for MRD analysis (n 33) uMRD is achieved with fixed-duration dosing: uMRD was achieved by C4 in most patients who achieved a CR Duration Progression-free (known) Initial treatment BOR and status CR PD MRD responses Undetected Detected All evaluable patients that achieved a CR had uMRD at the end of treatment MRD kinetics are consistent with observed durable responses BOR C4 uMRD/tested C8 uMRD/tested CR 93% (28/30) 100% (28/28) 73% (24/33) samples had detectable MRD prior to dosing Detection threshold 1e-6 6 12 18 24 30 36 Duration (months) 42 Exploratory analysis using ClonoSeq in patient PBMC collected longitudinally during and post mosunetuzumab treatment. BOR, best overall response; MRD, minimal residual disease; PBMC, peripheral blood mononuclear cells; uMRD, undetectable MRD. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 0
Conclusions In heavily pre-treated patients with R/R FL, fixed-duration mosunetuzumab is well-tolerated and can achieve long-lasting remissions – Durable responses with 3 years of follow-up: the estimated 30-month DOR rate was 73% in patients with a CR – A 3-year OS rate of 82% – A manageable safety profile with outpatient administration No new AEs were reported in this extended follow-up – Retreatment efficacy data are encouraging with mosunetuzumab Pharmacodynamic evaluation supports fixed-duration treatment – B-cell recovery is detectable at a median of 18.4 months after the end of treatment Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 – Deep molecular responses occur early; all patients in CR have uMRD at C8
Acknowledgments The patients and their families The study investigators The study coordinators and nurses The sponsor, Genentech, Inc. Schuster SJ, et al. ASH 2023 #603 M-DE-00019686 Third party medical writing assistance, under the direction of all authors, was provided by Aisling Lynch, PhD, and Deirdre Kelly, PhD, of Ashfield MedComms, an Inizio company, and was funded by F. Hoffmann-La Roche, Ltd
Doing now what patients need next