Housing First: Basic Principles Gregg Pieples Greater Cincinnati






















75 Slides1.99 MB
Housing First: Basic Principles Gregg Pieples Greater Cincinnati Behavioral Health Services [email protected] Andy Hutzel Over-the-Rhine Community Housing [email protected] Fred Baxter Greater Cincinnati Behavioral Health Services [email protected]
Community Mental Health Agency Founded in 1971 350 employees Serves approximately 6000 individuals per year Services offered: Psychiatric Care Management Specialized Care Management (Homeless, Court) Counseling Vocational Day Program Integrated Health Care – Nursing, medical care, pharmacy services
Projects for Assistance in Transition from Homelessness (PATH) – Homeless Outreach PATHS TO RECOVERY Uses Housing First Approach IDDT/ACT Team Integrated Behavioral Health Counselors in Health Care for Homeless Site Housing First ACT Team Uses Housing First Approach GCB Homeless Services
Project Partners Mental Health Greater Cincinnati Behavioral Substance Abuse Alcoholism Council Housing OTRCH Evaluation SARDI - Wright State University
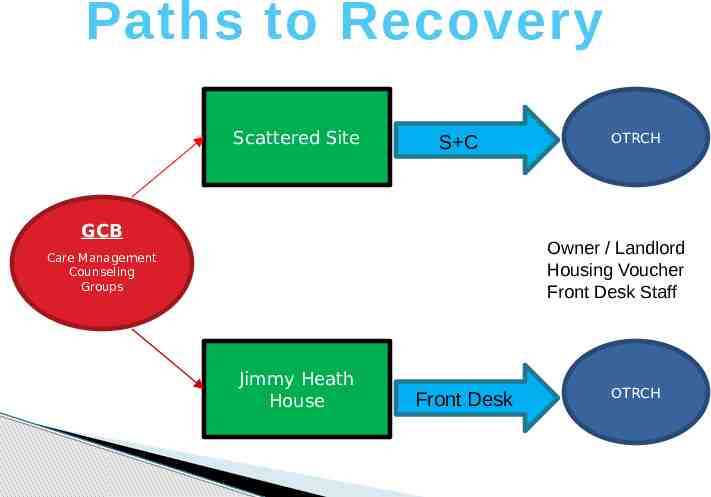
Paths to Recovery Scattered Site S C GCB OTRCH Owner / Landlord Housing Voucher Front Desk Staff Care Management Counseling Groups Jimmy Heath House Front Desk OTRCH
Overview n he t By rg Ta be m u P et op rs t io a l u 93 Admissions to date 75 current units of housing 25 Congregate units (JHH) 48 Scattered-site units n Chronically homeless Chronic Public Inebriates Multiple arrests Failed Treatment Hx Non-service connected Currently using Currently homeless Official Start Date: October 2009
WHAT IS HOUSING FIRST A consumer driven housing and support service that offers people who are homeless immediate access to an apartment of their own and the services needed for recovery.
Housing First programs may be constructed in a number of ways, but share the following features: The direct, low barrier placement into permanent housing No requirement to complete another program first Provision of intensive, readily available support services Although participation in these services is not required Sobriety is not a requirement Use of Evidence based practices (EBP) Continued services regardless of previous or continued failures Consumer driven
Why Housing First? SAMHSA / HUD priority Housing First is an "evidence-based practice,“ Multiple research studies report that HF programs consistently show significant positive impact on its target population Longer stays in Housing Reduced substance use Less hospitalizations and incarcerations Impact of using a Housing First methodology at Pathways to Housing Showed significant housing retention rates and lower substance use rates as compared with traditional Contiuum of Care programs. Autonomy & Control. Perceived choice was much higher in Housing First. The Streets to Homes program in Toronto housed more than 1,500 people since inception 87 percent have remained housed. Reduction in the use of Substances, emergency services such as 911, emergency rooms, ambulance, fire, police detox, and jail
Pathways Housing First (PHF) "Some people think when you give housing away that you’re actually enabling people as opposed to helping them get better. Our experience has been that the offer of housing first, and then treatment, actually has more effective results in reducing addiction and mental health symptoms, than trying to do it the other way. The other way works for some people, but it hasn’t worked for the people who are chronically homeless." Sam Tsemberis Founder & CEO Pathways to Housing
Variations of Original HF Design Variations occur in service type & intensity housing type Outcomes show consistency in Housing retention but vary in other areas Seattle vs. New York Models
Critical Elements of Housing First Separation of Housing & Treatment Client Choice of Housing & Services Intensive Treatment Services A Recovery Philosophy
Separation of Housing & Treatment Requires a change in Thinking
Separation of Housing & Treatment Housing Services Apply for housing subsidy Find apartment Using ACT or other Intensive Case Management Sign lease Maintain housing (abide by a lease) Supportive housing contact weekly Treatment and Support services Relapse (either MH or SA) is expected Does not result in housing loss Treatment Services
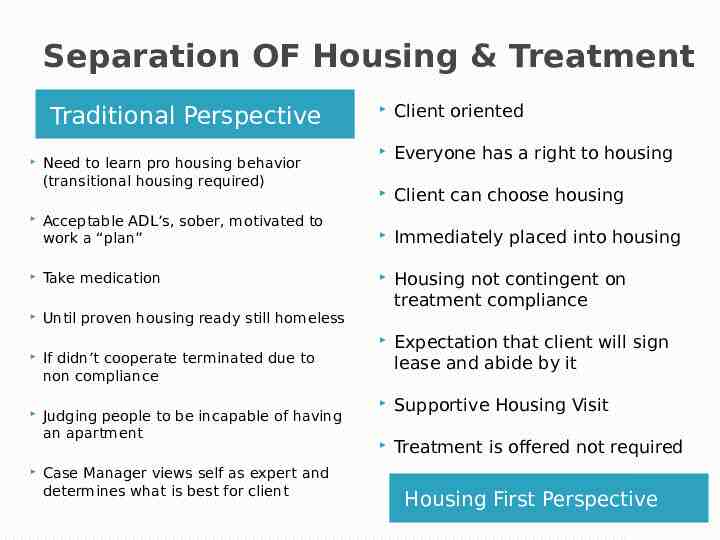
Separation OF Housing & Treatment Client oriented Everyone has a right to housing Client can choose housing Acceptable ADL’s, sober, motivated to work a “plan” Immediately placed into housing Take medication Until proven housing ready still homeless Housing not contingent on treatment compliance Expectation that client will sign lease and abide by it Supportive Housing Visit Treatment is offered not required Traditional Perspective Need to learn pro housing behavior (transitional housing required) If didn’t cooperate terminated due to non compliance Judging people to be incapable of having an apartment Case Manager views self as expert and determines what is best for client Housing First Perspective
INTENSIVE TREATMENT SERVICES ACT or Intensive Case Management Service
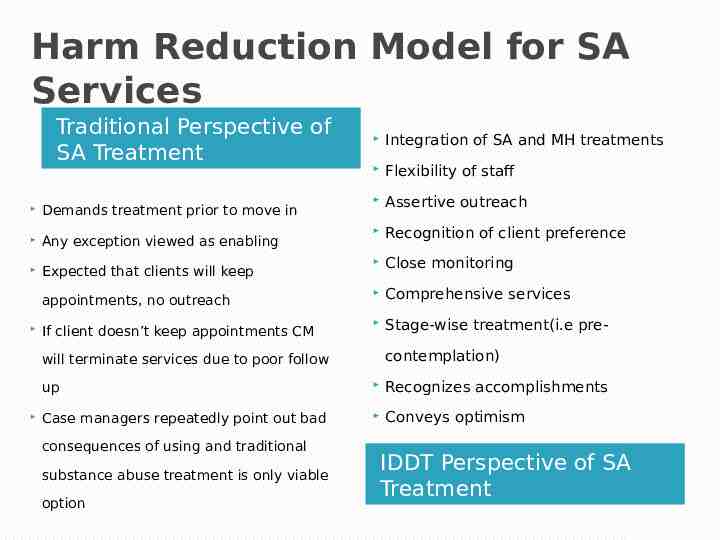
Harm Reduction Model for SA Services Traditional Perspective of SA Treatment Integration of SA and MH treatments Flexibility of staff Assertive outreach Recognition of client preference Close monitoring appointments, no outreach Comprehensive services If client doesn’t keep appointments CM Stage-wise treatment(i.e pre- Demands treatment prior to move in Any exception viewed as enabling Expected that clients will keep contemplation) will terminate services due to poor follow up Recognizes accomplishments Case managers repeatedly point out bad Conveys optimism consequences of using and traditional substance abuse treatment is only viable option IDDT Perspective of SA Treatment
CLIENT CHOICE OF HOUSING AND TREATMENT Choice is the foundation of Housing First
Client Choice Dignity of Choices Right to risk People make mistakes and learn from the experience Learn to ask what clients want Offer what housing options you have Client makes choice Clients typically want their own apartment Treatment Services are offered; not required
Landlords as Partners Landlord, Agency and Tenant have common goal Agency makes sure rent is on time Agency is responsive to landlord concerns Tenant Rights and Responsibilities-there are limits to choice Must sign lease Pay portion of Rent Abide by Lease
Scattered site Apartments Traditional Perspective Clients can fully integrate into community Clients with many needs require group settings Group settings often from everyone else Client has no choice in housing option case manager knows what is in the clients best interest Feels part of society and has increased sense of self have supervision 24/7 Can be indistinguishable worth Can feel they truly have own home Housing First Perspective
Client choice of treatment Traditional Perspective Case manager views self as the expert Client may reject any services except supportive housing visit Client determines frequency of service & sequence of service Focus on establishing trust by meeting needs as presented by client No strings attached Teaches responsibility no real choice Must take meds to get into housing Can’t work on any treatment goals unless sober Client chooses treatment goals & services determines what is best for client Manipulating client through coercion Must express they want treatment before moving into housing Cant transport if smells like alcohol Clients do not see consequences as their responsibility if they don’t see their choice use consequence of behavior as opportunity to learn Housing First Perspective
Recovery Philosophy Recovery is possible
Recovery Focused Services Convey Hope Offer choice after Choice Are respectful, patient, nurturing, compassionate Are strength based and client centered Move client toward independence Allows SA clients to determine what recovery is to them
Best Practices Importance of Evidenced Best Practices Housing First Integrated Dual Diagnosis Treatment Motivational Interviewing Trauma Informed Care Strengths Based Case Management
Motivational Interviewing Goes hand in hand with the Housing First Model
A collaborative, person-centered form of guiding to elicit and strengthen motivation for change February 2009 Revised definition Center for Evidence Based Practices Ohio SAMI CCOE What is Motivational Interviewing ?
Motivational Interviewing Listening with empathic understanding Evoking client’s own concerns/motivations Reducing resistance Nurturing hope & optimism
Guiding Principles Express Empathy Develop Discrepancy Roll with Resistance Support Self-Efficacy It’s about connecting to individuals that have made a habit out of not connecting
Stages of Change Precontemplation Contemplation Preparation Action Maintenance/Relapse Prevention Prochaska and DeClementi, Miller and Rollnick 1991 Ohio SAMI CCOE Regional Training
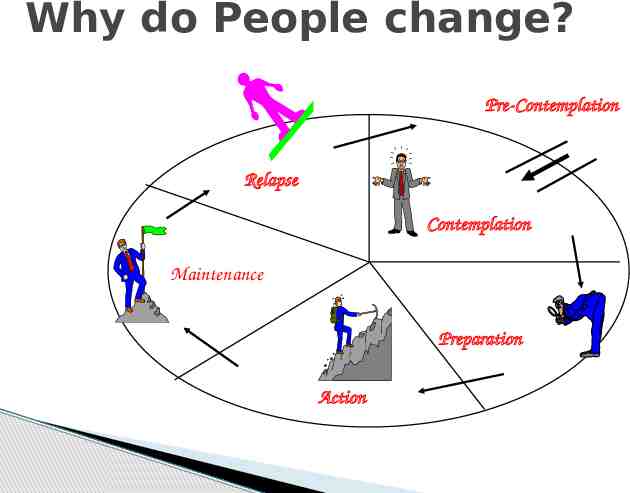
Why do People change? Pre-Contemplation Relapse Contemplation Maintenance Preparation Action
Stages of Change & Stages of Treatment Pre-contemplation Engagement Contemplation & Preparation Persuasion Action Active treatment Maintenance Relapse Prevention Ohio SAMI CCOE Regional Training
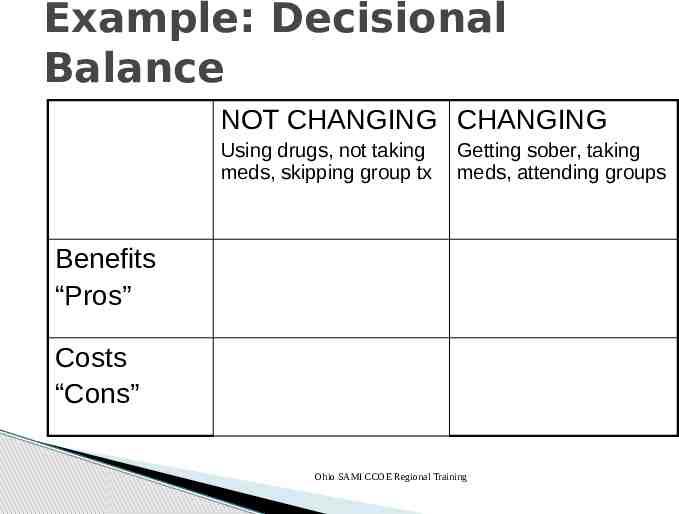
Example: Decisional Balance NOT CHANGING CHANGING Using drugs, not taking meds, skipping group tx Getting sober, taking meds, attending groups Benefits “Pros” Costs “Cons” Ohio SAMI CCOE Regional Training
P2R Services Fred Baxter MSW, LSW Clinical Counselor
Team and Services Team 5 FTE’s Program Manager Counselor Two Care Managers Peer Specialist Data person Services Housing Support Care Management Counseling Crisis Intervention Groups Peer Mentoring
Care management Basic Needs Housing Support Cleanliness Safety Communication with Landlord Lease obligations Benefits Food Clothing Medical care Vocational Social Supports
Counseling Non-Traditional Setting Often not in office Style Rarely a sit-down Length Very short sessions
Engagement Strategies Dialogue & Topic commonality Assessment Groups Treatment Referrals Individual Rapport Building Trust through demonstration
Groups Engagement by Nature Support and Education Coordination of Services
Group Guidelines Respect Others Able to participate Intoxicated members Highly symptomatic members
Group Structure Welcome Topics Open Flexible Examples Connection Announcements Coordination News Educational Segment What is hope? Cultural Diversity Community Safety
Group Tenets Group is voluntary Relational Staff and client connected Group patterns and counseling must consider the members interest, motivation and cognitive ability
Program Criteria A review of the population
Chronic Public Inebriate Chronic homelessness Chronic alcoholism Multiple arrests Failed Treatment Hx Non-service connected Currently using Currently homeless
Importance of Collaboration Selection Committee Committee Members Monthly Meeting DIC All potential Clients HIP Team Reviewed Cincinnati Police Prioritized DCI (Chico / Valerie) OTRCH PATH
Historical View
History of Project Need for a response to the long-term shelter stays Affectionately known as the “keep alives” 2004 2007 Multiple sites reviewed for possible construction Public dissent Corporate community disapproved of the model Project delays and stoppage
Project History Community Task Force InterAct for Health HUD SSH Funds Awarded 2006
SAMHSA Grant Services Agencies Design & Implementation 2009
Outcome Data
Demographical overview of clients (N 91) 91.2% male 52.7% African American / 45.1% Caucasian Average age 50.11 years 11.0% Veterans 60.4% completed 12th grade 97.8% unemployed
Living situation before Paths to Recovery 34.1% 65.9% Shelter Street/Outdoors
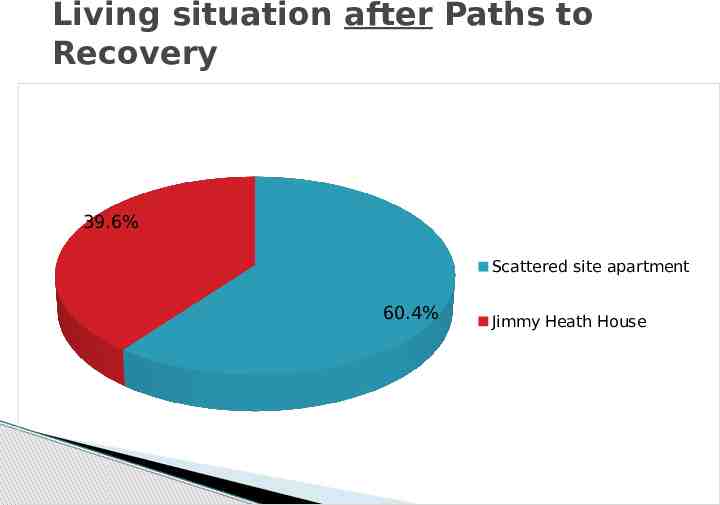
Living situation after Paths to Recovery 39.6% Scattered site apartment 60.4% Jimmy Heath House
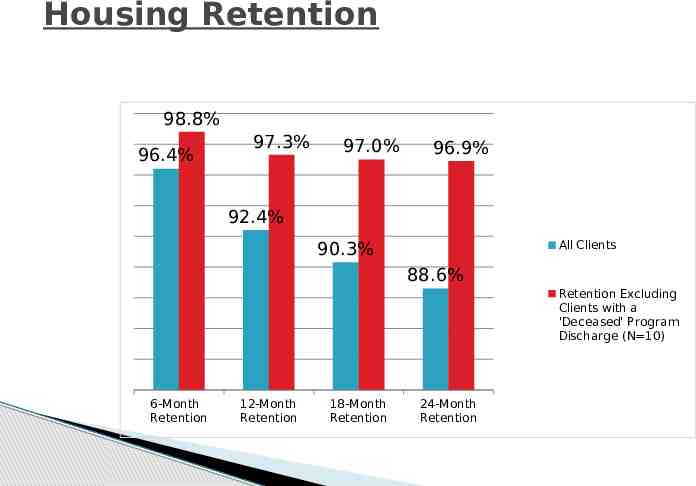
Housing Retention 98.8% 96.4% 97.3% 97.0% 96.9% 92.4% All Clients 90.3% 88.6% Retention Excluding Clients with a 'Deceased' Program Discharge (N 10) 6-Month Retention 12-Month Retention 18-Month Retention 24-Month Retention
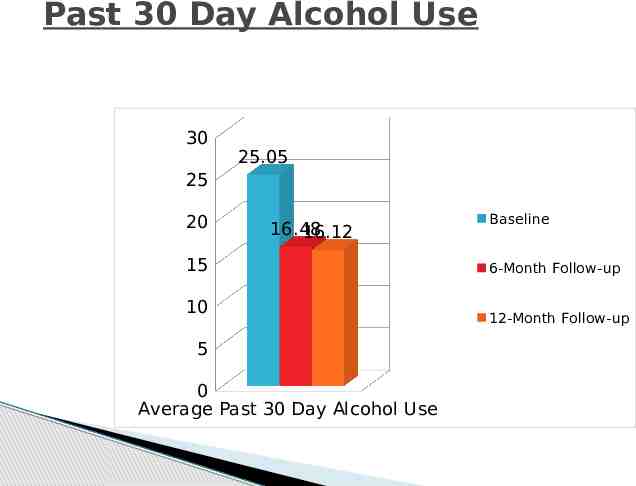
Past 30 Day Alcohol Use 30 25.05 25 20 16.48 16.12 15 10 5 0 Average Past 30 Day Alcohol Use Baseline 6-Month Follow-up 12-Month Follow-up
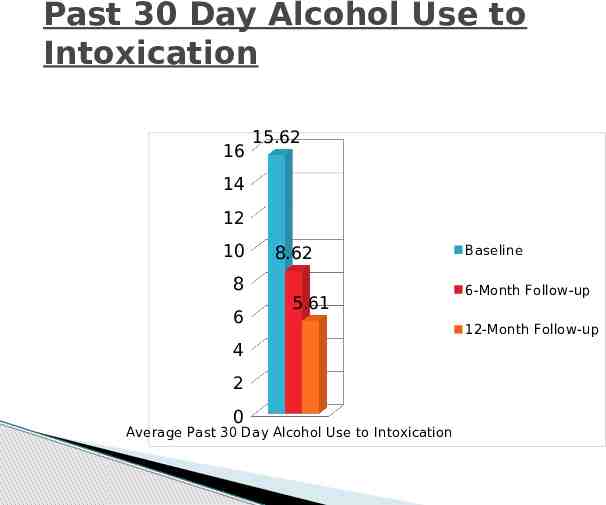
Past 30 Day Alcohol Use to Intoxication 16 15.62 14 12 10 8 6 8.62 5.61 4 2 0 Average Past 30 Day Alcohol Use to Intoxication Baseline 6-Month Follow-up 12-Month Follow-up
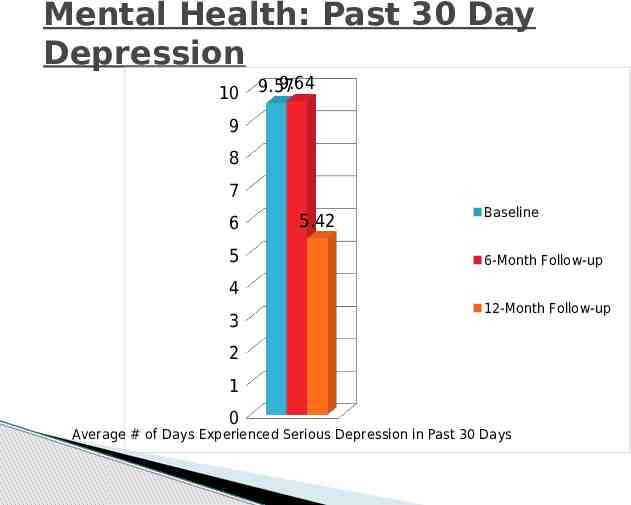
Mental Health: Past 30 Day Depression 10 9.64 9.57 9 8 7 6 5 5.42 Baseline 6-Month Follow-up 4 3 12-Month Follow-up 2 1 0 Average # of Days Experienced Serious Depression in Past 30 Days
Criminal Justice Activity Arrest and confinement data Obtained from the Hamilton County Clerk of Courts 57 clients Criminal justice data Obtained for the 24-month period before and after housing placement
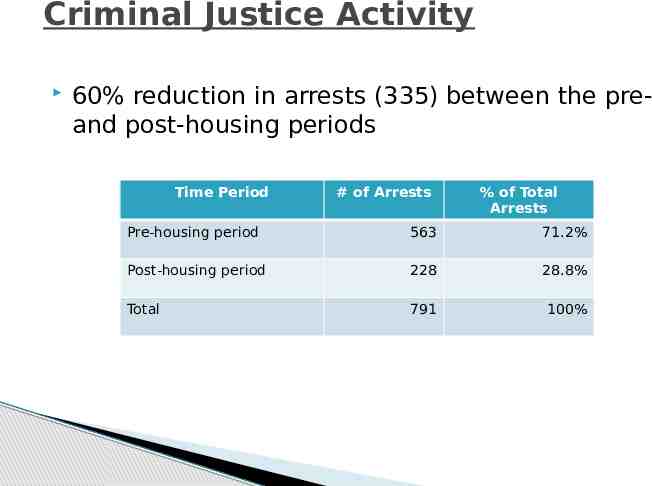
Criminal Justice Activity 60% reduction in arrests (335) between the preand post-housing periods Time Period # of Arrests % of Total Arrests Pre-housing period 563 71.2% Post-housing period 228 28.8% Total 791 100%
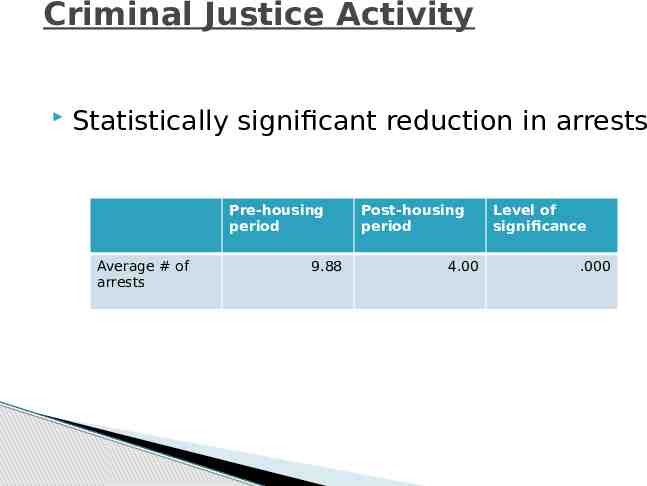
Criminal Justice Activity Statistically significant reduction in arrests Pre-housing period Average # of arrests 9.88 Post-housing period 4.00 Level of significance .000
Criminal Justice Activity 44% reduction in jail days between the pre- and post-housing periods 642 fewer jail days in the post-housing period Time Period Pre-housing period Post-housing period Total # Days Confined % of Total Confinement 1456 64.1% 814 35.9% 2270 100%
Criminal Justice Activity No statistically significant reduction in jail days
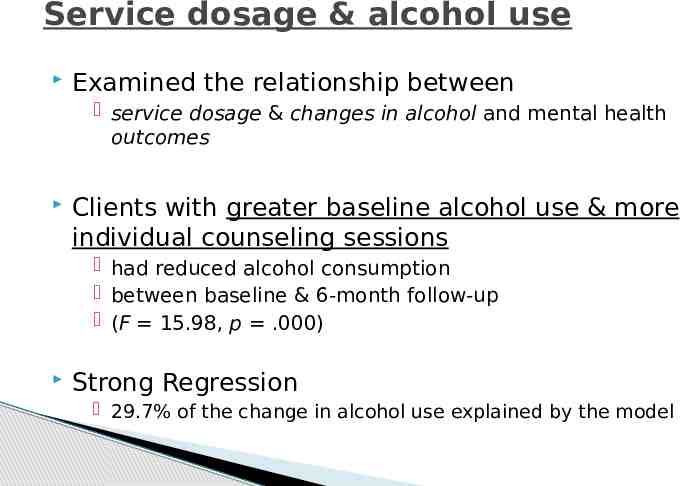
Service dosage & alcohol use Examined the relationship between service dosage & changes in alcohol and mental health outcomes Clients with greater baseline alcohol use & more individual counseling sessions had reduced alcohol consumption between baseline & 6-month follow-up (F 15.98, p .000) Strong Regression 29.7% of the change in alcohol use explained by the model
Program Successes Excellent housing retention Sustained reductions in alcohol use Reduced criminal justice activity Low staff turnover Strong, continued partnerships Active participation in services 97.7% 85.2% 80.7% 85.2%
Property Management Operations
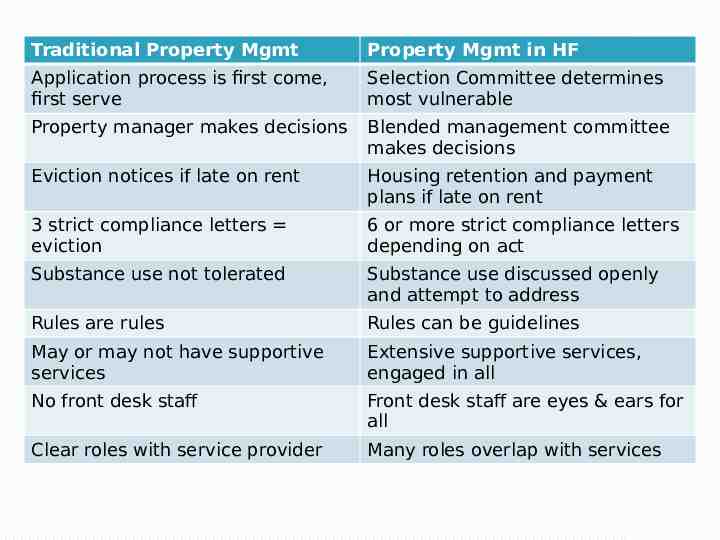
Traditional Property Mgmt Property Mgmt in HF Application process is first come, first serve Selection Committee determines most vulnerable Property manager makes decisions Blended management committee makes decisions Eviction notices if late on rent Housing retention and payment plans if late on rent 3 strict compliance letters eviction 6 or more strict compliance letters depending on act Substance use not tolerated Substance use discussed openly and attempt to address Rules are rules Rules can be guidelines May or may not have supportive services Extensive supportive services, engaged in all No front desk staff Front desk staff are eyes & ears for all Clear roles with service provider Many roles overlap with services
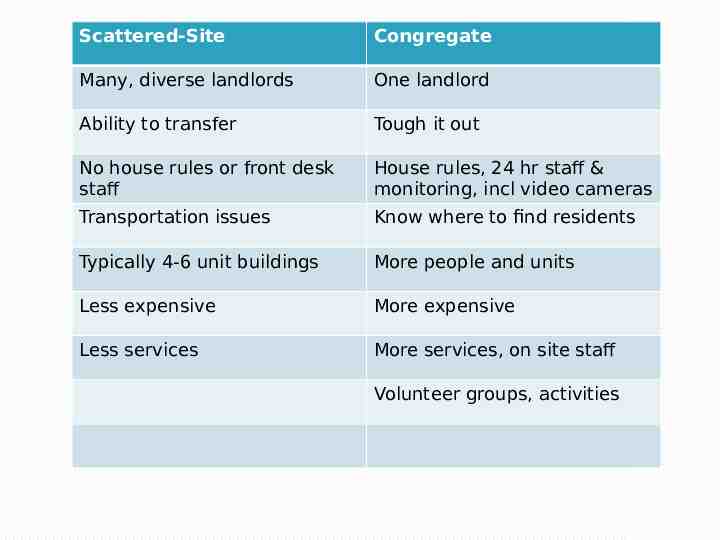
Scattered-Site Congregate Many, diverse landlords One landlord Ability to transfer Tough it out No house rules or front desk staff House rules, 24 hr staff & monitoring, incl video cameras Transportation issues Know where to find residents Typically 4-6 unit buildings More people and units Less expensive More expensive Less services More services, on site staff Volunteer groups, activities
Lessons Learned
Lessons Learned Communication and teamwork Measure success in years, not weeks or months Housing First for the 10th time Difficult decisions Every Housing First project is a bit different Be creative in addressing issues Chronic illness much greater than anticipated Patience is critical Staff morale is ongoing concern
Lessons Learned Try to be a helper rather than a policeman. Even when dealing with very difficult behavior, most people are doing the best they can (at the moment). They are up against their limitations. “When I knew better, I did better” Services need to be individualized and focus on the particular needs of the client. Clients can demonstrate the same behavior with very different etiologies. Trauma and mental illness are often the occult cause of negative behavior, substance abuse may take center stage and be the most apparent issue but it may not be the source of the issue. It is difficult for homeless individuals to transition into permanent housing. We frequently see men and women who have been “housed” for years remain a “Homeless Person” in their mind.
Lessons Learned Assess carefully –clients are frequently having cognitive issues or suffering from dementia from long term substance abuse. Harm Reduction needs to be the center of the approach to individuals in housing first programs When working with actively using addicts, interventions should first focus on the negative behavior, not the addiction it’s self. It’s not the substance abuse in and of it’s self , it’s the behavior. Not all negative behavior is based on addiction. One should look at social skills, competency, physical limitations, cognitive abilities. Many clients do not have basic coping skills or ability to manage a household. Chronic means chronic issues will reoccur
Feedback And small group exercise
References 1. Centers for Disease Control and Prevention. (1999). Framework for Program Evaluation in Public Health. Morbidity and Mortality Weekly Report, 48(RR11), 1-40.
Other Resources 1. Substance Abuse and Mental Health Services Administration. Permanent Supportive Housing: Evaluating Your Program. HHS Pub. No. SMA-10-4509, Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services, 2010. 2. Burt, M.A. (2004). The Do-It-Yourself Cost-Study Guide. Assessing Public Costs Before and After Permanent Supportive Housing: A Guide for State and Local Jurisdictions. Corporation for Supportive Housing.
Exercise – Small Group Most difficult to house client What are the barriers to successful housing? What are some strategies to overcome those barriers Would any HF principles assist in the process?





