Policy Recommendations for the March Virtual House of Delegates as

25 Slides6.99 MB
Policy Recommendations for the March Virtual House of Delegates as of January 31, 2024
The House of Delegates Ultimate authority over ASHP professional policies One annual session consisting of 2 in-person meetings at the June House of Delegates and 3 virtual meetings (March, May, and November) The House considers professional policy proposals that have been approved by the Edit Master text styles Board of Directors Second level Third level Fourth level Fifth level Most of these professional policy proposals are contained in reports from ASHP councils but may come from other component bodies, delegates, or ASHP members
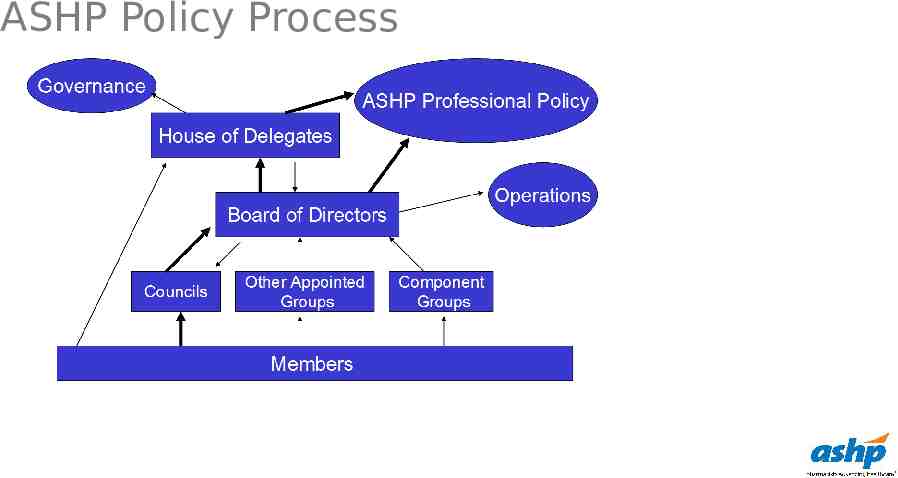
ASHP Policy Process
March Virtual House of Delegates The policy recommendations in the following slides are scheduled to be considered at the March virtual House of Delegates. If any of those policy recommendations are not approved, they will be considered at the June House meeting. Proposed policies are found on the House of Delegates website and are debated on the ASHP House of Delegates Connect community by delegates and other ASHP members. It is important to review the Board Reports on Policy Recommendations for each meeting (found on the House of Delegates website) because that report provides a rationale and background information not found on ASHP Connect. All ASHP members, including delegates, are encouraged to use the ASHP House of Delegates Connect community to review and comment on any of the proposed policies. Web-based discussion in advance of a House meeting may influence how delegates vote, and it also permits delegates to discuss potential amendments before the June House.
CPhP: Role of the Pharmacy Workforce in Improving Mental Health To advocate for equitable and destigmatized access to mental healthcare services for all patients across their lifespan, including members of the healthcare workforce; further, To affirm the essential role of pharmacists, as members of the interprofessional care team, in increasing patient access to mental healthcare services; further, To urge all members of the pharmacy workforce to raise awareness of, screen for, triage, and provide education on mental health conditions; further, To advocate for expansion of mental health-related comprehensive medication management services provided by pharmacists; further, To advocate for adequate funding of mental health awareness
CPhP: Independent Prescribing Authority To affirm that prescribing is a collaborative process that includes patient assessment, understanding of the patient’s diagnoses, evaluation and selection of available treatment options, monitoring to achieve therapeutic outcomes, patient education, and adherence to safe and cost-effective prescribing practices; further, To recognize that pharmacists are highly trained medication experts on the interprofessional care team capable of making independent and autonomous evidence-based decisions on medication therapy management; further, To advocate that pharmacists have independent and autonomous authority to initiate, modify, and deprescribe all schedules and classes of medications; further, To advocate that healthcare delivery organizations establish credentialing and privileging processes for pharmacists that delineate scope of practice, support pharmacist prescribing, and ensure that pharmacists who prescribe are accountable, competent, and qualified to do so; further, To advocate that all pharmacists have a National Provider Identifier that is recognized by payers. Note: This policy would supersede ASHP policies 2236 and 2251.
CPhP: Suicide Awareness, Prevention, and Response To support the goal of zero suicides; further, To collaborate with key stakeholders in support of suicide awareness, prevention, and response; further, To acknowledge that optimal suicide awareness, prevention, and response efforts focus both on patients and on the healthcare workforce; further, To recognize that pharmacists, as key members of the interprofessional care team, are integral to suicide awareness, prevention, and response efforts, and to acknowledge the vital role of other members of the pharmacy workforce in those efforts; further, To foster the use and development of clinically validated tools to aid the pharmacy workforce in assessing the influence of medications and other factors on suicidality; further, To advocate for adequate government and healthcare organization funding for suicide awareness, prevention, and response; further, To enhance awareness of local, state, national, and global suicide awareness, prevention, and response resources. Note: This policy would supersede ASHP policy 1901.
CPhP: Pharmacist’s Role on Ethics Committees To advocate that pharmacists should be included as members of, or identified as a resource to, hospital and health-system ethics committees; further, To encourage pharmacists to actively seek ethics consultations or solicit input from their institution’s ethics committee, as appropriate; further, To encourage pharmacists serving on ethics committees to seek advanced training in healthcare ethics. Note: This policy would supersede ASHP policy 1403.
CPhP: Safe Handling and Administration of Hazardous Drugs To advocate that pharmaceutical manufacturers eliminate surface contamination on packages and vials of hazardous drugs (HDs); further, To inform pharmacists and other personnel of the potential presence of surface contamination on the packages and vials of HDs; further, To advocate that all healthcare settings proactively conduct an interprofessional assessment of risk for exposure to HDs during handling and administration, including the use of closed-system transfer devices (CSTDs); further, To advocate for pharmacist involvement in the development of policies, procedures, and operational assessments regarding administration of HDs, including when CSTDs cannot be used; further, To advocate that the Food and Drug Administration require standardized labeling and package design for HDs that would alert handlers to the potential presence of surface contamination, including development of CSTD-compatible, ready-to-administer HD products; further, To encourage healthcare organizations, wholesalers, and other trading partners in the drug supply chain to adhere to published standards and regulations. Note: This policy would supersede ASHP policies 1615 and 1902.
CPuP: Order Verification To advocate that a prescriber should not be solely responsible for medication ordering, dispensing, and administration as well as any patient monitoring and evaluation, except when a double check would limit patient access to care.
CPuP: Liability Protection To advocate that pharmacists be able to provide evidence-based dispensing and care to patients without fear of criminal or civil legal consequences, harassment, or liability; further, To advocate that protection against liability extend to referrals for out-of-state care and for dispensing to patients from another state.
CPuP: State Prescription Drug Monitoring Programs To support continued state implementation of prescription drug monitoring programs that collect real-time, relevant, and standard information from all dispensing outpatient entities about controlled substances and monitored prescriptions; further, To advocate that such programs seek adoption into health information exchanges to best integrate into electronic health records and to allow prescribers, pharmacists, and other practitioners to proactively monitor data for appropriate assessment and dispensing; further, To advocate that such programs improve their interstate data integration to enhance clinical decision-making and end-user satisfaction; further, To encourage policies that allow practicing pharmacists to gain access to databases without holding licensure in each state; further, To promote research on the effects of prescription drug monitoring programs and electronic health record programs on opioid prescribing, dispensing, misuse, morbidity, and mortality. Note: This policy would supersede ASHP policy 1408.
CPuP: Emergency Supplies of Drug Products To discontinue ASHP policy 1906, Emergency Supplies of Drug Products, which reads: To advocate for states to allow any pharmacist, during a declared emergency, to dispense without a prescription an emergency supply of a drug product in quantities that meet the needs of patients.
CPuP: Drug Nomenclature To discontinue ASHP policy 9011, Drug Nomenclature, which reads: To work with the FDA, USP, and pharmaceutical industry to assure that drug products are named in a manner that clearly and without confusion permits identification of ingredients’ strengths and changes.
COT: Medication Stewardship Programs To advocate that pharmacists are foundational members of any medication stewardship program; further, To affirm that pharmacists bring unique clinical, operational, safety, and financial expertise to help organizations develop and manage medication stewardship programs; further, To promote pharmacist leadership in medication stewardship teams; further, To encourage healthcare organizations to develop comprehensive medication stewardship programs that align with applicable laws, regulations, and accreditation standards; further, To support incorporation and development of the pharmacy workforce in medication stewardship efforts; further, To enhance awareness that medication stewardship includes disease state management across all levels of care and addresses barriers at
COT: Nonprescription Status of Rescue and Reversal Medications To support the over-the-counter (OTC) status of medications intended for evidence-based rescue use or reversal of potentially fatal events; further, To work with federal, state, and local governments and others to improve the rescue and reversal medication development and supply system to ensure an adequate and equitably distributed supply of these medications; further, To advocate that all insurers and manufacturers maintain coverage and limits on out-of-pocket expenditure so that patient access to rescue and reversal medications is not compromised; further, To support and foster standardized education and training on the role of rescue and reversal medications and their proper administration, safe use, and appropriate follow-up care.
COT: Research on Drug Use in Obese Patients To discontinue ASHP policy position 1920, Research on Drug Use in Obese Patients, which reads: To encourage drug product manufacturers to conduct and publish pharmacokinetic and pharmacodynamic research in obese patients to facilitate safe and effective dosing of medications in this patient population, especially for medications most likely to be affected by obesity; further, To encourage manufacturers to include in the Food and Drug Administration (FDA)– approved labeling detailed information on characteristics of individuals enrolled in drug dosing studies; further, To advocate that the FDA develop guidance for the design and reporting of studies that support dosing recommendations in obese patients; further, To advocate for increased enrollment and outcomes reporting of obese patients in clinical trials of medications; further, To encourage independent research on the clinical significance of obesity on drug use, as well as the reporting and dissemination of this information via published literature, patient registries, and other mechanisms; further, To recognize that pharmacists are medication therapy experts who should provide guidance on appropriate drug dosing for obese patients.
COT: Therapeutic Interchange To discontinue ASHP policy 8708, Therapeutic Interchange, which reads: To support the concept of therapeutic interchange of various drug products by pharmacists under arrangements where pharmacists and authorized prescribers interrelate on the behalf of patient care.
CEWD: Flexible Workforce Models To advocate for flexible workforce models that promote patient safety and continuity of care, optimize pharmacy operations, and enhance recruitment and retention of the pharmacy workforce.
CEWD: Pharmacy Residency Training To continue efforts to increase the number of ASHPaccredited pharmacy residency training programs and positions available; further, To promote efforts to increase recruitment and retention of residents in ASHP-accredited pharmacy residency programs; further, To encourage stakeholders to evaluate priority areas within pharmacy for future residency training needs. Note: This policy would supersede ASHP policy 0917.
CPM: Pharmacist Access to Provider Networks To advocate for laws and regulations that require healthcare payers to include pharmacists in their provider networks as standard coverage when providing patient care services within their scope of practice and the services are covered benefits; further, To advocate that payers provide comparative, transparent sharing of performance and quality measure data for all providers in their networks, including pharmacists. Note: This policy would supersede ASHP policy 2134.
CPM: Risk Assessment of Health Information Technology To urge hospitals and health systems to directly involve departments of pharmacy in performing appropriate risk assessment before new health information technology (HIT) is implemented or existing HIT is upgraded, and as part of the continuous evaluation of current HIT performance; further, To advocate that HIT vendors provide estimates of the resources required to implement and support new HIT; further, To collaborate with HIT vendors to encourage the development of HIT that improves patient-care outcomes and user experience; further, To advocate for changes in federal law that would recognize HIT vendors’ safety accountability. Note: This policy would supersede ASHP policy 1418.
CPM: Unit Dose Packaging Availability To advocate that pharmaceutical manufacturers provide all medications used in health systems in unit dose packages or, when applicable, in packaging that optimizes medication safety, improves operational efficiency, and reduces medication waste; further, To urge that the Food and Drug Administration require pharmaceutical manufacturers to provide stability data to support the repackaging of medications outside of their original manufacturer bulk containers in the interest of public health, healthcare worker and patient safety, and reduced waste. Note: This policy would supersede ASHP policy 2253.
CPM: Optimizing the Medication-Use Process To discontinue ASHP policy 9903, Optimizing the Medication-Use Process, which reads: To urge health-system pharmacists to assume leadership, responsibility, and accountability for the quality, effectiveness, and efficiency of the entire medication-use process (including prescribing, dispensing, administration, monitoring, and education) across the continuum of care; further, To urge health-system pharmacists to work in collaboration with patients, prescribers, nurses, and other health care providers in improving the medication-use process.
Questions or Suggestions? Feel free to contact: Melanie Dodd, Chair, ASHP House of Delegates: [email protected] ASHP policy website: https://www.ashp.org/Pharmacy-Practice/Policy-Positions-and-Guidelines/