HCA 660 Christina McClenaghan Dwane McGowan Matthew


19 Slides328.35 KB
HCA 660 Christina McClenaghan Dwane McGowan Matthew Mabalot COMPUTERIZED PROVIDER ORDER ENTRY (CPOE) PROJECT PLAN
AGENDA Project Overview Value Provided to Customers Project Scope and Limitations Deliverables for Pilot Project Timeline Tactical Plan Gantt Chart Risk Matrix Budget Q&A
VISION STATEMENT To ensure that the Midwest Health Care Group continues to be a regional leader, excelling in the provision of safe, quality, cost effective, and timely care for our patients. We must also strive to provide a workplace for our staff and physicians that is the envy of all health care groups. Implementation of a key meaningful use (MU) core objective such as CPOE will allow the full potential of the existing electronic health record system to take effect, reducing costly errors, improving patient safety, decreasing mortality and morbidity rates, and avoiding duplication of tests. It will save our group financially by reducing administrative staff costs, improving billing practices, and increase the transaction processing rate. This project will be implemented in phases, with the first implementation occurring as a pilot at one of our primary care clinics.
PROJECT OVERVIEW Midwest Health Care Group will benefit from the implementation of a CPOE system in the following ways: 1) Improved clinical decision-making in conjunction with existing HER and DSS technology. 2) Reduction in medication errors and associated costs. 3) Improved patient safety. 4) Decreased length of stay in hospital. 5) Workflow process improvement. 6) Compliance with federal requirements for Stage II of meaningful use. 7) Improved physician clinical staff satisfaction over time. 8) Reduction/elimination of paper orders and legibility issues.
PROJECT OBJECTIVES The project has the following major objectives: 1) Implementation of a pilot Clinical Provider Order Entry system at one of the systems primary care clinics that meets or exceeds MU requirements. 2) Creation of a unified implementation road map for eventual expansion of CPOE throughout all campuses of the Midwest Health Care Group. 3) Development of clinical order sets, alerts, and protocols. 4) Development of downtime procedures for planned/unplanned downtime. 5) Creation of key documentation for staff use during/following implementation. 6) Identification of resources required to maintain and expand CPOE at MHCG in the future. 7) Develop capabilities to capture data in order to produce required reports (public health reporting).
VALUE PROVIDED TO CUSTOMERS Conformance to physician outlines standard practice Increased use of evidence-based medicine Increased patient safety Improved productivity Reduction of duplicate services Improved reporting on public health issues
PROJECT SCOPE AND LIMITATIONS Scope of Initial Release The initial implementation of CPOE will be limited to one facility, using a pilot project approach to identify issues before going system-wide. It will involve nursing, radiology, physicians, pharmacy, and administration as appropriate. Workplace realignment, workflow, and physical reconfiguration of work spaces should also be a consideration.
PROJECT SCOPE CONTINUED Interface Scope The vendor should be guaranteeing that the system selected for implementation will be capable of interfacing with the existing EHR system, although the same vendor is being used so this shouldn’t be an issue. Organizational Scope The implementation is to be as a pilot project initially, to identify any areas of concern.
PROJECT SCOPE CONTINUED Organizational Scope The implementation is to be as a pilot project initially, to identify any areas of concern. Conversion Scope The conversion process should involve: 1) Converting existing data to new system format, ensuring the data is complete, accurate, and current. 2) IS staff should take the lead, with input from end-users (clinical, administrative). 3) Use of a system of validation checkpoints for accuracy and reliability after conversion. 4) Testing with live data, involving IS, vendors, end-users, and administrative staff as appropriate.
PROJECT SCOPE CONTINUED Scope of Subsequent Releases Subsequent implementation of this CPOE system is subject to executive approval and successful roll-out of this pilot project. Out of Scope Billing functions are not within the scope of this implementation. Scheduling and registration are not in the scope of the scope of the current implementation. Cleaning up backlog of maintenance request for order entry improvements and enhancements. Physicians’ non-order documentation Structured notes Flowsheets
DELIVERABLES Team Charter Project Definition Plan Budget Plan Weekly status report to client PowerPoint presentation Final Report
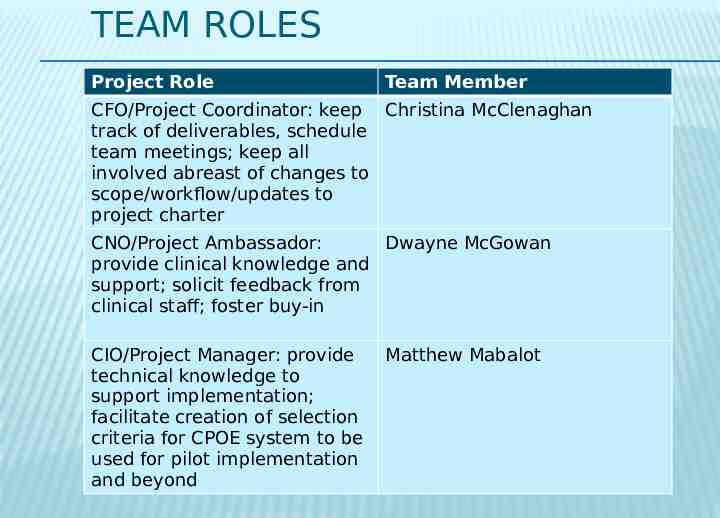
TEAM ROLES Project Role Team Member CFO/Project Coordinator: keep Christina McClenaghan track of deliverables, schedule team meetings; keep all involved abreast of changes to scope/workflow/updates to project charter CNO/Project Ambassador: Dwayne McGowan provide clinical knowledge and support; solicit feedback from clinical staff; foster buy-in CIO/Project Manager: provide technical knowledge to support implementation; facilitate creation of selection criteria for CPOE system to be used for pilot implementation and beyond Matthew Mabalot
TIMELINE Initiate planning on 03/11/13 and present project plan to the board on 03/28/13. Upon Approval, the Pilot Project will commence on 07/30/13 and be completed by 12/01/13 . Approximate date of completion of major phases: 07/30/13
TACTICAL PLAN GANTT CHART
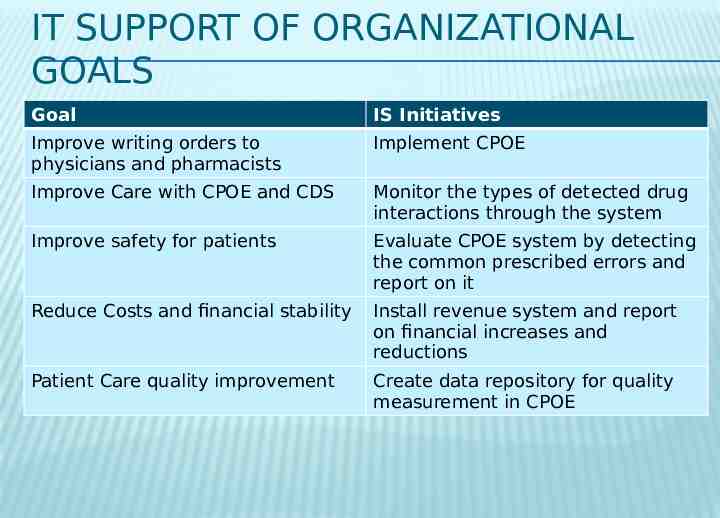
IT SUPPORT OF ORGANIZATIONAL GOALS Goal IS Initiatives Improve writing orders to physicians and pharmacists Implement CPOE Improve Care with CPOE and CDS Monitor the types of detected drug interactions through the system Improve safety for patients Evaluate CPOE system by detecting the common prescribed errors and report on it Reduce Costs and financial stability Install revenue system and report on financial increases and reductions Patient Care quality improvement Create data repository for quality measurement in CPOE
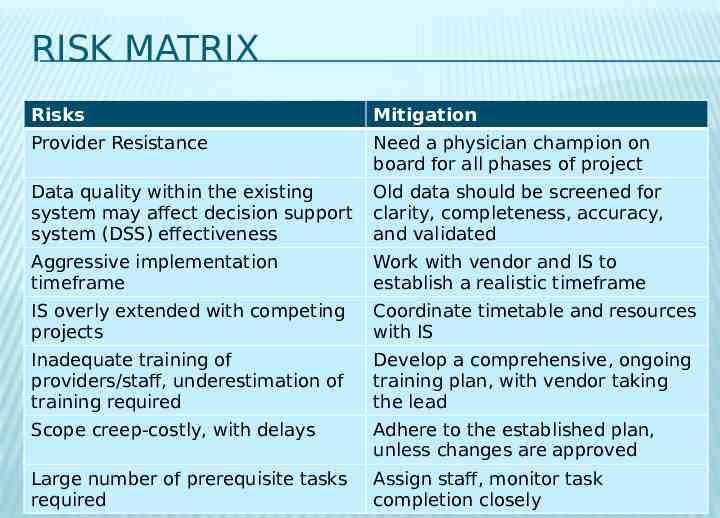
RISK MATRIX Risks Mitigation Provider Resistance Need a physician champion on board for all phases of project Data quality within the existing system may affect decision support system (DSS) effectiveness Old data should be screened for clarity, completeness, accuracy, and validated Aggressive implementation timeframe Work with vendor and IS to establish a realistic timeframe IS overly extended with competing projects Coordinate timetable and resources with IS Inadequate training of providers/staff, underestimation of training required Develop a comprehensive, ongoing training plan, with vendor taking the lead Scope creep-costly, with delays Adhere to the established plan, unless changes are approved Large number of prerequisite tasks required Assign staff, monitor task completion closely
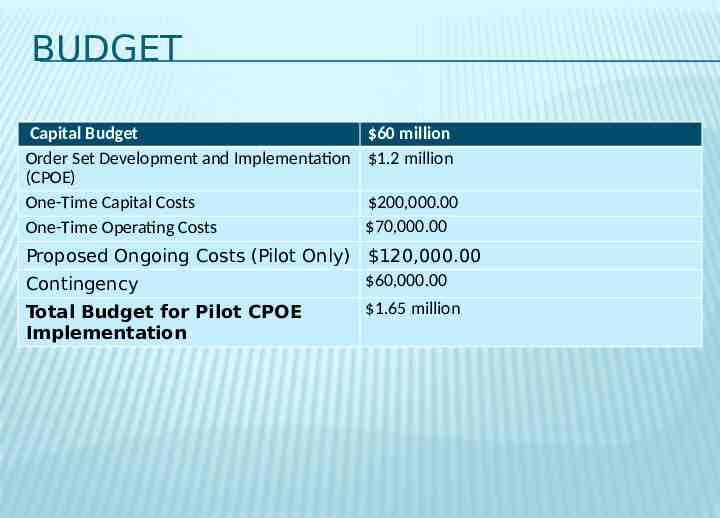
BUDGET Capital Budget Order Set Development and Implementation (CPOE) One-Time Capital Costs One-Time Operating Costs 60 million 1.2 million 200,000.00 70,000.00 Proposed Ongoing Costs (Pilot Only) 120,000.00 60,000.00 Contingency Total Budget for Pilot CPOE Implementation 1.65 million
UPCOMING MILESTONES Upon approval, The CPOE project organization team will begin executing the project by designing the process system and developing the CPOE application. Once the design is complete and the team is satisfied with result, the team will conduct full system testing and complete user testing. The team will then monitor and control the application including training throughout the implementation.
Q&A