EMR for Research: OTTR vs ? The Good, The Bad, and the Unknown














































67 Slides421.77 KB
EMR for Research: OTTR vs ? The Good, The Bad, and the Unknown Laurel Williams, RN, MSN, CCTC OUI Conference 10/1/2013 Omaha, Nebraska
Disclosures I have no financial disclosures (darn it!) I am no computer expert (ask Dr. Shaw) I am an advocate to do the right thing for patients and families I like simple and I’m partial to OTTR I am a University of Michigan grad but a Huskers fan (when they aren’t playing U of M)
Objectives Describe the use of OTTR and EMR in clinical research involving transplant patients Provide examples of the use of OTTR in clinical transplant research Provide examples of EMR use in clinical transplant research
Historical Background OTTR Liver Transplant Program at UNMC started 6/1985 Patient records hand written, kept in multiple note books Computerized records would: -improve accuracy of patient data/patient care -allow more access to information for patient care(xrays, lab results, reports etc flowing to one source) -save time, tell pt story, identify what “we” do Enter OTTR/Intuacare designed to be supportive
Historical Background 2010 Health Reform Law Affordable Care Act: Improve quality of care-pay for performance not volume increase competition, regulation, incentives Improve access to care – No preexisting conditions, no caps, young adults stay longer on parent policy
Historical Background EMR HITECH ACT (Health Information Technology for Economic and Clinical Health) Part of American Recovery and Reinvestment Act 2009 Not about healthcare reform Goal to have portable electronic record Decrease fraud and misuse of Medicare/Medicaid funds Assure payments are accurate for service and documented Establish financial incentives to hospitals – meaningful use measures (HHS attempting to align
What About Research? One of EMR Measures of Success Ability to generate list of patients by specific conditions to use for : Improve Quality Reduction of disparities (treat everyone equally) Research Outreach
Research Done Using OTTR The Lived Experience of Parents and Guardians Providing Care for Their Children who Have Undergone Transplantation Williams, L.; Eilers, J.; Heerman, J.; Smith, K. (2012) Progress in Transplantation. 22(4): 393-402 The Impact of Solid Organ Transplantation on Primary Care Givers: A Cross Sectional Pilot Study Williams, L.; Eilers, J.; Brown, J.; Snell, L.; Sorrell, J.H.
Research Using OTTR/EMR Evaluation of Post Solid Organ Transplant Patient Education for Continuous Quality Improvement Williams, L.; Eilers, J., Keck, M.; Lecci, K; Snell, L. Interventions to Decrease the Impact of Post-Operative Ileus After Liver Transplant or Resection Surgery Williams, L.; Botha, J.; Davis, G.; Vannausdle, S.; Eilers J. Uncertainty Management Interventions for Patients Awaiting Liver Transplantation Williams, L. Site PI; Baily, C., Study PI (Duke University) Parents of Pediatric Organ Recipients; Transition to Home and Chronic Illness Care Williams, L. Site PI; Larret, S., Study PI (Children’s Hospital of Wisconsin)
The Lived Experience Of Parents/Guardians Providing Care For Their Children Who Have Undergone Transplantation What are we doing and can we do it better? Laurel Williams, RN, MSN, CCTC University of Nebraska Medical Center NATCO 35th Annual Meeting August 1, 2010 Hollywood, Florida
Are We Missing Something? Case I 14 month old post L/SB/P transplant Young parents feeling “stressed out” at time of evaluation due to chronic illness (unmarried) Returned home 4 months post transplant Hard to reach mom – missed labs/MD appts (broken water pipes at home) Local MD “fired” mom/pt due to difficulties
Case I continues Noon – mom reports child is fine 1700 – mom reports child lethargic with multiple water loss stools and fever Instructed to go immediately to ER 2030 Child arrives in ER – unstable/dry Cardiac arrest and death Time at home – 2 weeks
Are We Missing Something Case 2 14 month old post L/SBP transplant Single mother Returned home 4 months post transplant Small community hospital/limited resources admit for cytogam – hard to find accepting MD Trouble reaching mom by phone (no long distance) Financial issues (car problems, formula)
Case 2 Continues Missed lab work and MD appointments Fluctuating Prograf levels CPS referral – provide more resources Starts to vomit and sent to ER Instructed by ER MD to start clear liquids and sent home
Case 2 Continues Child becomes more lethargic at home Taken to grandparents house Vomiting continues and child stops breathing CPR initiated in the home – 911 called Child dies in the ER Time at home 6 months
Background Intestinal transplantation offers hope for children facing life threatening illness One year survival rates 81% at some centers Expensive, complex process with the majority of children being cared for at home Highly technical cares that in the past would have been provided by healthcare professionals
Background Improved survival at what cost (QOL) Given life-threatening nature of transplant: parents may experience increased stress, compromise their own emotional health, and their ability to care for their children Parents face increased responsibilities at home (loss of Transplant Center support network)
Background Parent and social relationships may become disrupted in the months and years post transplant Less social support at home once acute crisis of hospital and surgery completed Studies have begun to examine the psychological distress of children post transplant but not in their parents
What Does the Literature Tell Us? Survival rates are improving Studies needed to look at impact on survivors and caregivers Few reports in the literature addressing the impact on parents and families
Study Goals Describe the lived experience of parents/guardians who have served as primary caregivers for children post solid organ transplant - Describe their experiences preparing for and providing care to children post dismissal - Identify the perceived needs of the caregivers - Provide preliminary data to guide future to improve quality of care provided
Sample 37 letters of invitation mailed 7 responses (5 accepted, 2 declined) 5 interviews completed 1 unable to access by phone (despite consent) 1 letter requesting no more contact 7 undeliverable 23 no response
Demographics Subject 1 Subject 2 Subject 3 Subject 4 Subject 5 Age 50-69 19-30 19-30 50-69 31-49 Relations Foster Mother Mother* Mother* Grandfath er Mother SE Status 40-50,000 10,000 1020,000 8099,000 4059,000 Education Some College Less than HS Some College 4yr College 2yr College Marital Status Widowed Single Married Married Married Child Age – Tx 11 months 13 months 11 months 17 months 6.7 yrs Type TX L/SB/P L/SB/P L/SB/P SB only SB only Age at Death 3.6 years 22 months 16 months 6.4 years 7.4 years Survival 9 months 5.5 months 5 years 2.7 years * Mothers pregnant during time of transplant 9 months
Theme Perception of Team Interactions Communications –10-12 people on rounds shooting questions back and forth. “Parents kind of get left aside.” –“Holy crap, I wasn’t able to ask my questions” Have to chase team down the hall to get answers (“ping ping, ping down the halls”) –Takes time for us to know team and they us. We had to “learn their language” –Need to be heard – didn’t know completely how to say things –If you don’t like the answer ask someone else
Theme Parents Perceptions of Team Interactions Relationships One physician always stayed to answer questions One physician nonchalant- wanted more human side as child became more ill Nurses would come back only if looked puzzled Families lean on other families for support – might not be getting the right information “You guys are their family, so to speak, their extended family and they come to depend on you for emotional and professional support.”
Theme Parents Perception of Team Interactions Process (what helped in transition home) - Local MD and hospital - Coordinators/NP’s and staff – overall knowledge - Having numbers for team and home health care - Finding a system to help organization
Theme Parent Readiness to Go Home Doctor’s told me I was ready I had everything clear when I came back I felt pretty comfortable We had been taught pretty well Needed more information of meds and “all that good stuff. At the time I wasn’t prepared to have all the information” Felt thrilled but apprehensive; happy but nervous Expect the worst
Theme Parents Perception Interactions with Local Care Systems Communications LMD thought he was prepared- not for severe px Knowing how to communicate problems – “She didn’t have pain but was in a funk” Have to keep telling them to give the meds on time “They (LMD) didn’t listen to me”. They thought they were the doctors and knew better LMD afraid to call the Transplant Center. “They will think they are not good doctors” Do they(LMD) know when to send pt back?
Theme Providing Care for Patient and Self Need to be vigilant, even when pt in the hospital Need to care for child, even if it affects adult friends or family relationships with “less regard for self” “Sleep with one eye open.” “Buck up and fight a little harder” Accept medical needs as normal; organize home Need to experience normal childhood activities Comfort level changes with new care needs
Conclusion Parents and guardians of child transplant recipients do have experiences that could contribute to stress Stress involves perceived inconsistencies that exist within the transplant program Stress involves perceived differences between transplant and local care teams Stress involves parents need to provide most of the hands-on care In preparing parents for discharge we must be aware of the differences between what we communicate and how it is interpreted
Ongoing Questions How do we teach parents our language and should we need to? How do we teach parents all the signs and symptoms of possible problems? How do we teach parents to be persistent? How do we prepare parents to be confident? How do we reach local care providers who are not normally involved in transition home?
Study Limitations Small pilot size Care providers responding may not be typical of our patient population (single, younger, lower SE status not reflected in data)
The Impact of Solid Organ Transplantation on Primary Caregivers: A Cross Sectional Pilot Study Transplantation is the treatment of choice for many patients with end-stage organ failure With adequate survival data, studies start to look at what happens to survivors and their families Studies have shown that care givers are at risk for depression, anxiety and post traumatic stress Less stressed caregiver offers more beneficial post transplant support
Purpose To determine the impact of solid organ transplantation on primary caregivers at different time intervals post transplantation (3-5 months; 6-8 months, and 12-14 months). To identify factors that may influence the impact on caregivers of post transplant patients at stated time intervals To determine the feasibility of using the selected instruments in future longitudinal studies
Subjects 19 years of age or greater who speak and understand English Primary care provider of an abdominal organ transplant recipient as mutually identified by the patient and care provider Goal of 30 participants in each interval
Methods/Instruments Anxiety/Depression Post Traumatic Stress Care Giver Appraisal of Health Social Support Psychological Adjustment to Illness Phone Interviews with subset of subjects
Preliminary Findings Male caregivers have more depression and anxiety than female caregivers Female caregivers have more perceived social support from friends and family than male caregivers Female caregivers more likely to seek out information than male caregivers No PTSD reported by any caregiver One subject showed clinical symptoms of PTSD
Implications for Practice Examine our interactions with caregivers, especially male caregivers Be careful to avoid gender bias Look more closely at protective factor of gender for female care providers
Evaluation of Post-Solid Organ Transplant Patient Education for Continuous Quality Improvement Laurel Williams RN, MSN, CCTC Lecia Snell, RN, MSN, Megan McCartan, PharmD, BCPS, Kassandra Lecci, PharmD, June Eilers, PhD, APRN-CNS, BC 19th Annual ITNS Symposium and General Assembly October, 2010 Minneapolis, Minnesota
Project Rationale 15-30% of transplant recipients exhibit medication non-adherence1 Regimen complexity and perceived benefits from therapy affect medication adherence Self-management patient education has been shown to improve self-efficacy reduce health-care utilization Multidisciplinary approach is key and includes good communication techniques
Phase I Methods Phase II Nursing Data Collection PT Transplanted Nursing Data Collection PT Transplanted PT transferred to floor PT transferred to floor Discharge Medication Teaching Daily MedActionPlanTM provided to PT/CG MedActionPlanTM provided to PT/CG Discharge Medication Teaching Outpatient Clinic Visit Updated MedActionPlanTM provided to PT/CG Outpatient Clinic Visit DC T
MedActionPlanTM 41
Study Criteria Prospective, observational pilot study Inclusion criteria: 19 years or older, able to speak and comprehend English Caregiver available and willing to participate Nursing – All staff nurses on the Solid Organ Transplant Unit Exclusion criteria: Non-English speaking, re-transplantation
Project Objectives Improve Pt/CG pre-discharge medication knowledge Evaluate Pt/CG and staff nurse satisfaction with the MedActionPlanTM teaching tool Identify post-discharge educational needs of transplant Pt/CGs Obtain baseline date on staff nurse perceptions of current standard of practice regarding discharge medication Evaluate staff nurse level of comfort teaching Pt/CGs about discharge medication Evaluate customized DCTTM program and relationship based care 43
% of Medication Questions Answered Correctly Results: Phase I 100% 80% 84% Pre-Discharge 60% 40% 82% 55% 43% 20% 0% PT CG Clinic
Results: Phase II % Medication Questions Answered Correctly 100% 80% 93% 86% 83% 90% 95% 97% 95% 60% Pre-Discharge Clinic 40% 20% 0% PT CG
Results: Phase I-II-III Medication Questions Answered Correctly by Patients 100% 90% 80% 82% 83% 86% 82% 80% 70% Hospital Clinic 60% 50% 40% 43% 30% 20% 10% 0% Phase 1 Phase 2 Phase 3
Results: Phase I-II-III Medication Questions Answered Correctly by Caregivers 100% 90% 90% 80% 92% 94% 88% 82% 70% 60% Hospital Clinic 60% 50% 40% 30% 20% 10% 0% Phase 1 Phase 2 Phase 3
Conclusions Phase I Pt/CG medication knowledge improved post discharge Pt/CG understanding is difficult to assess Phase II Daily inpatient medication charts: Improved medication knowledge pre-discharge Actively engaged the Pt/CG in the plan of care Prepared the Pt/CG to ask meaningful questions Phase III Pt/CG knowledge remained higher in both phases II and III from Phase I
From Raising the Rafters to Raising the Roof: Dale Carnegie TrainingTM Enhances Relationship Based Care Relationship based care (RBC) involves care of self, patient/family (pt/fam) and peers Nursing interactions significantly influence pt/fam satisfaction Patient education involves both technical and non technical skills Skilled sensitive communication is a defining feature of nursing core values, yet good communication techniques have “all but disappeared”.
From Raising the Rafters to Raising the Roof: Dale Carnegie TrainingTM Enhances Relationship Based Care Purpose Evaluate how the use of an abbreviated, customized Dale Carnegie TrainingTM (DCT) Program focusing on non technical skills, enhances relationship based care Sample 27 Staff RNs on the Solid Organ Transplant Unit Research Methods Customized DCT focusing on non technical skills Certified trainer – 3.5 hour classes every other week x 3 DCT is time-spaced and interactive involving learning, practice and feedback
DCT Customized Modules Module 1. Increased Self Confidence Focus in people as individuals Become familiar with human relations principles Communicate clearly and concisely with impact Module 2. Energize our Communications Be more natural when communicating with others Discover how relationships help us advance toward our goals, Concentrate on the strength of others Module 3. Communicate to Lead Create opportunities for feedback Demonstrate effective listening/questioning skills Consider various forms of communication and their impact
Results Self Rating Pre & Post Testing Ranges 1-10 Pre mean Postmean Growth Self Confidence 6.5 8.2 26% Human Relations 6.6 8.5 28% Communication 6.5 8.5 30% Team Building 6.6 8.3 25% Stress/Attitude 5.8 7.9 37%
Nursing Comments after DCT Better communication with patients and families Improved listening skills More comfortable in getting to know pt/fx Improved working relations with staff More trust Appreciated strengths of co-workers Better speaker in front of group Better cooperation Better attitude/less stress Improved unit and organization reputation – increased quality care
Conclusions Skills promoting RBC are crucial for enhancing quality care DCT enhances and promotes the use of RBC skills by: Building self confidence Developing positive interactions Assuring communications are effective and delivered with impac Creating leaders DCT enhances RBC with will impact the quality of delivered care and the image of the organization
Interventions To Decrease the Impact of Post-Operative Ileus after Liver Transplant or Resection Surgery (The Poop Study) Clinical Trials.gov #NCT01156129 Laurel Williams, RN, MSN, CCTC University of Nebraska Medical Center NATCO 37th Annual Meeting Washington, DC August 15, 2012
What is Post-Operative Ileus (POI)? Temporary paralysis of a portion of the intestine Multi-factorial Causes including: Decreased electrical activity in GI tract due to anesthesia and opioid medications Electrolyte imbalance Manipulation of the bowel Local inflammation Often under reported
Traditional Interventions Avoidance of oral intake (NPO) Decompression of the stomach (NG) Reduction in use of opioids Early ambulation Pro-motility drugs (not effective) Center/Team specific protocols
Consequences of POI Increased pain Increased nausea & vomiting Possible aspiration pneumonia Gastric distension (hernia/wound dehiscence) Delayed ambulation (pneumonia/DVTs) Delayed feeding (malnutrition/delayed wound healing) Increased length of stay
How Bad Can It Really Be? In the United States, the economic impact of POI is estimated to be between 750 million and 1 Billion each year! Woodwad, Rastinehad, & Richstone (2008)
Study Purpose Purpose: determine the efficacy of interventions used in the early post operative period to enhance recovery from post operative ileus (POI) a. standard post-operative bowel management alone b. standard protocol plus the use of acupressure wrist bracelet for the management of nausea c. standard protocol plus sugarless gum chewing.
Methods and Subjects Design: Prospective, randomized-controlled trial (RCT) Subjects : 19 years or older, who speak and read English Scheduled for liver resection or transplant surgery Exclusion: Patient unable or unwilling to participate Withdrawal: Prolonged ICU stays, return to operating room, N/V greater than 3 days,
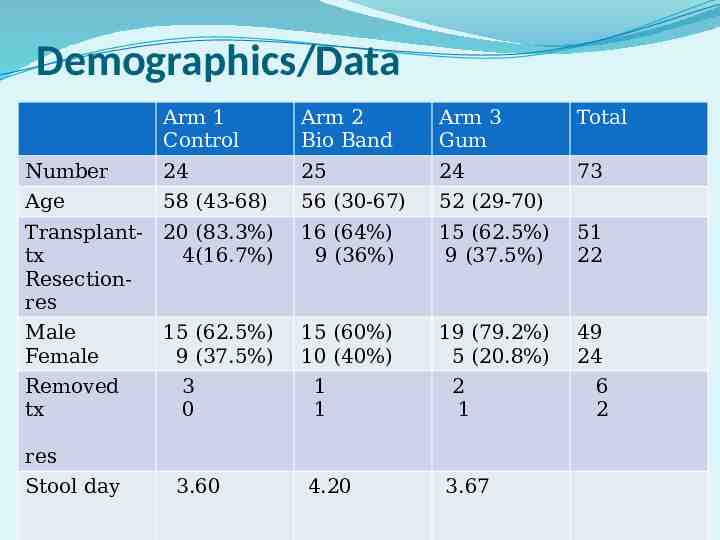
Demographics/Data Arm 1 Control Arm 2 Bio Band Arm 3 Gum Total Number 24 25 24 73 Age 58 (43-68) 56 (30-67) 52 (29-70) Transplanttx Resectionres 20 (83.3%) 4(16.7%) 16 (64%) 9 (36%) 15 (62.5%) 9 (37.5%) 51 22 Male Female 15 (62.5%) 9 (37.5%) 15 (60%) 10 (40%) 19 (79.2%) 5 (20.8%) 49 24 Removed tx 3 0 1 1 2 1 res Stool day 3.60 4.20 3.67 6 2
Findings - Stool Patterns Independent t-test Transplant Resection Day chart reports stool Day chart reports stool Mean 3.66 4.26 Observations 45 19 t Stat -1.51 P(T t) two tail 0.14 NS
Findings-Morphine Equivalents (mg) Independent t-test Transplant Resection MS Equivalents MS Equivalents Mean 123.62 509.62 Observations 46 18 t Stat -2.86 P(T t) one tail two tail 0.005 0.010 SS SS
Preliminary Conclusions Standard of care inconsistent across arms equally inconsistent across study groups No relationship between study arms, gender, type of surgery and day of first stool Transplant patients required significantly less MS equivalents than resection patients Patients reported satisfaction in using gum/less anxious No harmful effects of gum
EMR for Research: OTTR vs ? The Good, The Bad, The Unknown The Good – both “should” be able to allow quality research (if diagnosis codes/data are correct?) The Bad – At this time, the EMR seems cumbersome and does not capture “the whole story” The nation isn’t getting results that match its investment in healthcare (OWH, 8/25/13) The Unknown – Are their enough people to help with research projects, who know how to pull out the data? How will clinicians use the EMR for research? Will we continue to have the option of OTTR? We need to be at the table to an EMR that supports quality
Thank You OUI Nothing endures but change