ED Coding – Facility vs. Professional: It’s Different! GeBBS

12 Slides795.91 KB
ED Coding – Facility vs. Professional: It’s Different! GeBBS Healthcare Solutions
Scope It is important for coding professionals to understand the type of setting for the codes they are reporting. Facility fee coding Use of the room, lights, nursing staff, overhead costs for the facility Professional fee coding Complexity and intensity of providers work, including cognitive effort expended “Facility coding guidelines are inherently different from professional coding guidelines” - ACEP
Professional Fee Coding Evaluation & Management codes were developed in 1992 Congress established clear criteria (Documentation Guidelines) in 1995, additional revisions were introduced in 1997 Documentation guidelines (DG) recognize seven (7) components, three (3) of which are key components History Examination Medical Decision Making
Professional Fee Coding New patients require all three (3) of the key components to meet or exceed a level of service Established patients require only two (2) of the three (3) key components to meet or exceed a level of service No distinction is made between new and established patients in the emergency department Time is not considered a component for professional fee Evaluation & Management coding in the emergency department
Facility Coding Guidelines Since the implementation of the Outpatient Prospective Payment System (OPPS), the Centers of Medicare and Medicaid Services (CMS) required hospitals to report resources for emergency department visits using Evaluation & Management (E&M) codes. There is currently no national standard coding guidelines for facility E&M coding. CMS instructed hospitals to develop their own coding guidelines “Guidelines must reasonably relate the intensity of hospital resources to the levels of effort represented by the codes”
Facility Coding Guidelines CMS recognizes that the E/M level reported by the hospital will not necessarily match to the level of service reported by the physician for professional services provided for the same encounter. “Therefore, facilities should code a level of service based on facility resource consumption, not physician resource consumption. This includes situations where patients may see a physician only briefly, or not at all.”
Facility Coding: Four Basic Models CMS identified four (4) basic models in use when determining facility levels; Number or type of staff interventions Time Point system Patient severity Two of the most commonly used models for Emergency Department visit levels are the AHA/AHIMA Guidelines and the American College of Emergency Physicians ED Facility Level Coding Guidelines (ACEP Guidelines).
Facility Coding: Four Basic Models Number or type of staff interventions Intervention models use basic care interventions to report the lowest level of service, with higher levels assigned as complexity or number of nursing and ancillary staff interventions increases. AHA/AHIMA Guidelines and the ACEP Guidelines fall into this category. Time As time spent with the patient increases, so does the level assigned. Point system The time, complexity, and type of staff required determine the number of points assigned to each intervention. Patient Severity The diagnoses, level of medical decision making, and presenting complaint or medical problem are used to correlate resource consumption.
Eleven Criteria OPPS lists eleven (11) criteria that must be met for facility billing guidelines. The coding guidelines should follow the intent of the associated CPT code descriptor in that the guidelines should be designed to reasonably relate the intensity of hospital resources to the different levels of effort represented by the code. The coding guidelines should be based on hospital facility resources. The guidelines should not be based on physician resources. The coding guidelines should be clear to facilitate accurate payments and be usable for compliance purposes and audits. The coding guidelines should meet the HIPAA requirements.
Eleven Criteria The coding guidelines should only require documentation that is clinically necessary for patient care. The coding guidelines should not facilitate upcoding or gaming. The coding guidelines should be written. The coding guidelines should be applied consistently across patients in the clinic or emergency department to which they apply. The coding guidelines should not change with great frequency. The coding guidelines should be readily available for fiscal intermediary (or, if applicable, MAC) review. The coding guidelines should result in coding decisions that could be verified by other hospital staff, as well as outside sources.
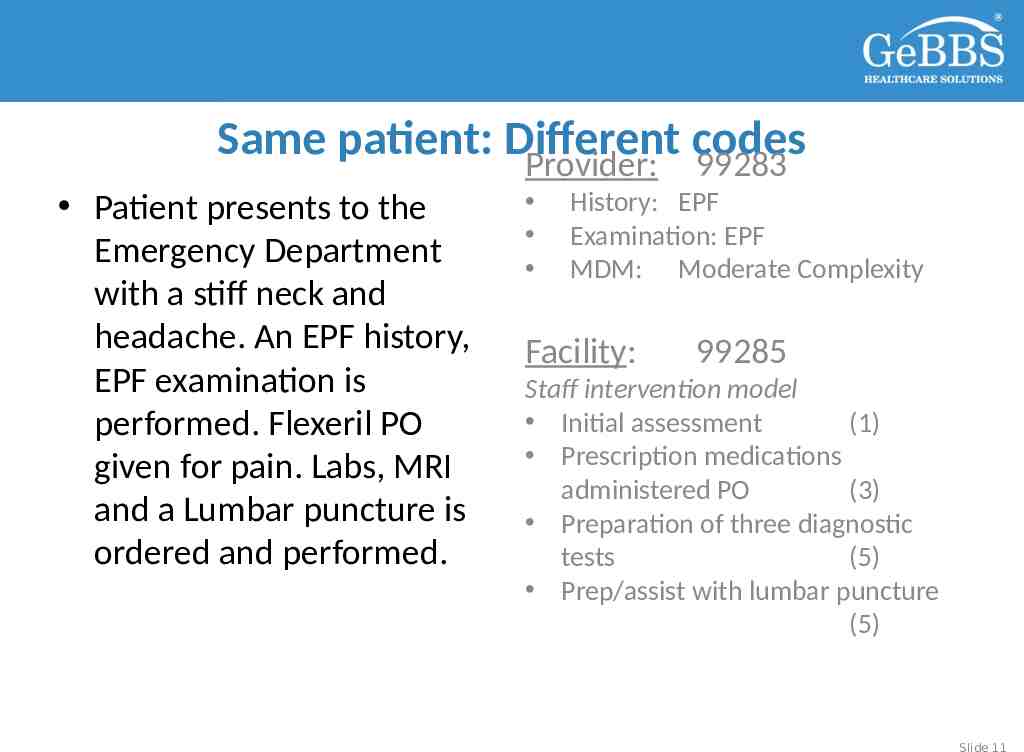
Same patient: Different codes Provider: 99283 Patient presents to the Emergency Department with a stiff neck and headache. An EPF history, EPF examination is performed. Flexeril PO given for pain. Labs, MRI and a Lumbar puncture is ordered and performed. History: EPF Examination: EPF MDM: Moderate Complexity Facility: 99285 Staff intervention model Initial assessment (1) Prescription medications administered PO (3) Preparation of three diagnostic tests (5) Prep/assist with lumbar puncture (5) Slide 11
Thank You! Cara Friederich 310.751.9567 [email protected] Slide 12