ECMO and Anticoagulation Brian C. Bridges, MD May 7, 2013

41 Slides1.78 MB
ECMO and Anticoagulation Brian C. Bridges, MD May 7, 2013
Coagulopathy Patients frequently have clotting abnormalities prior to initiating ECLS Disruption of hemostasis (fine balance between procoagulants and anticoagulants) – Activation of coagulation cascade requires anticoagulation to prevent thrombosis – Disruption and consumption of procoagulants requires its replacement to prevent bleeding
Platelets Need for platelet replacement steady for duration of ECMO Initial target platelet 80k Low platelet # is a risk factor for ICH (children and adults)
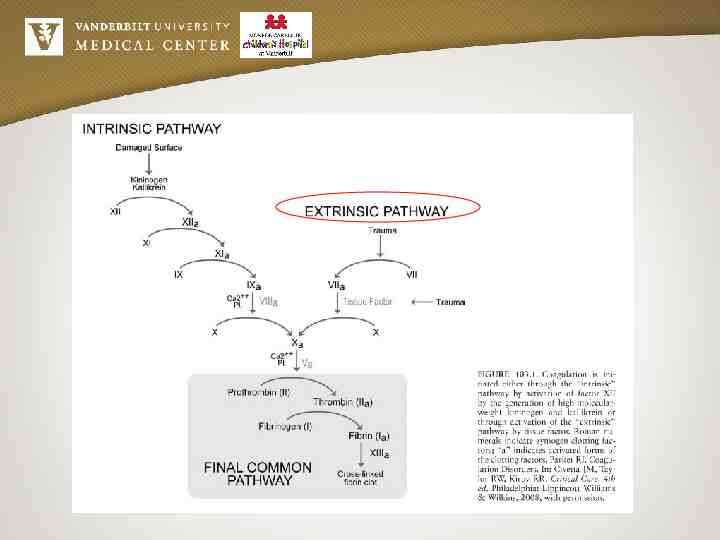
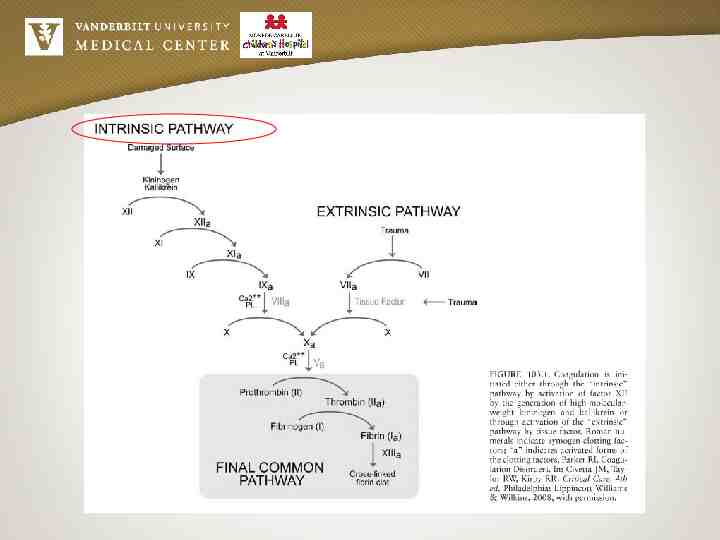
Coagulation Monitoring Prothrombin time (PT) – Assess the extrinsic pathway and final common pathway of clotting – Assess vitamin-K dependent factors (II,VII,IX,X) – Due to lab differences expressed as INR (international normalized ratio) – Heparin does not prolonged PT
Coagulation Monitoring Partial Thromboplastin Time (PTT) – Assess intrinsic and final common coagulation pathway – PTT is a plasma test activated by phospholipids which provides a measure of hemostasis in the absence of cellular components – Monitor heparin therapy – Assess only plasma component of heparin
Coagulation Monitoring PTT levels change significantly with age as part of developmental hemostasis PTT has poor correlation to anti-Xa levels in infants and children PTT seems to correlate better with unfractionated heparin concentration in adults
Coagulation Monitoring Activated Clotting Time (ACT) – Monitors coagulation of all blood components Platelet Plasma clotting factors – Crude method – Simple – Available at bedside Normal ACT 80–120 seconds Initial ECMO standard at Vanderbilt 200-220 seconds
Coagulation Parameters Hemoglobin, hematocrit, PT, INR, PTT, fibrinogen and platelets are monitored every 6-8 hours ACT measurements q1h at bedside Maintain hematocrit 30 to 40% Maintain platelets 80,000/mm3 INR goal depends on /- bleeding Maintain Fibrinogen 150 mg/dl
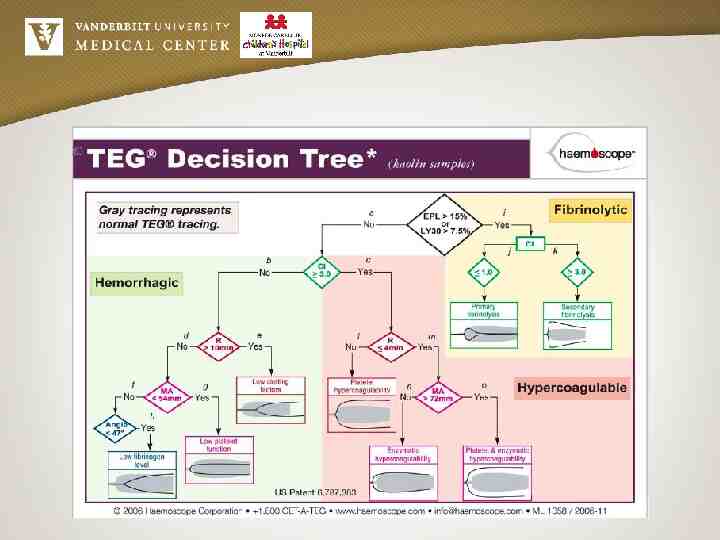
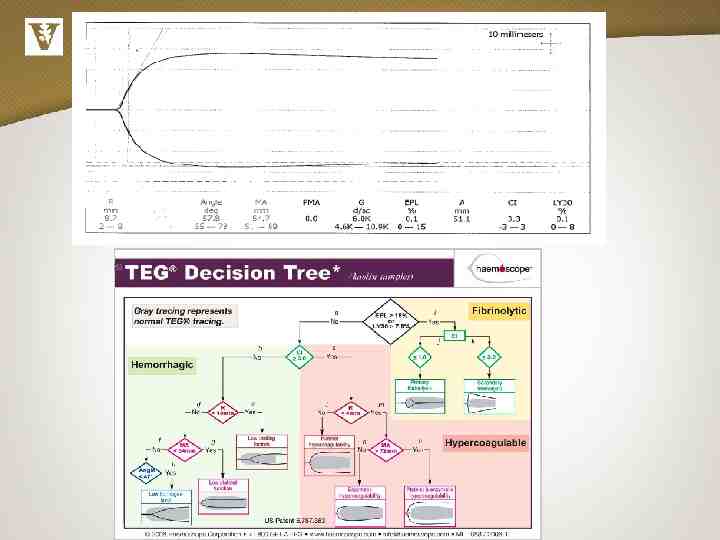
Coagulation Parameters Since September 2011, regularly following heparin assays (Anti X-a), AT3 levels QAM, and TEG PRN clotting or bleeding
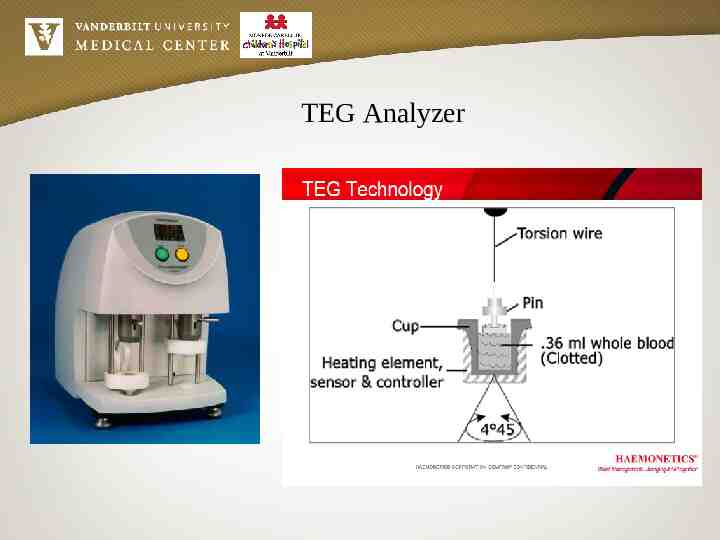
TEG Analyzer
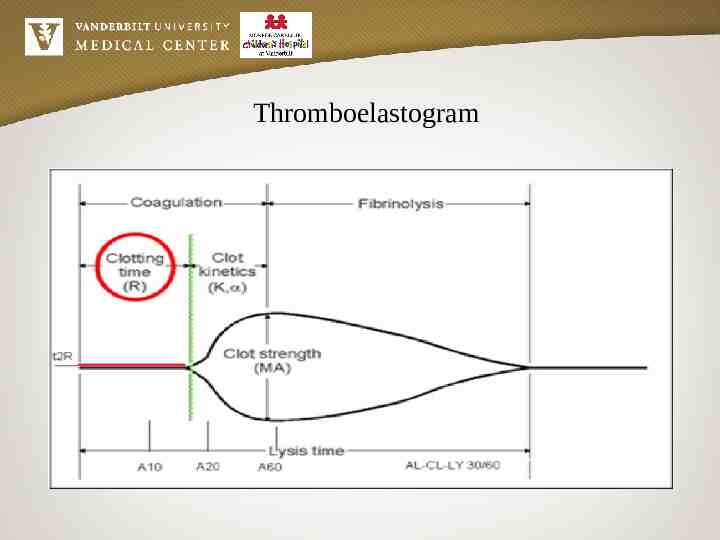
Thromboelastogram
Antithrombin Anthrombin is the primary physiologic inhibitor of in vivo coagulation, via inactivation of thrombin, plasmin, factor IXa, Xa, XIa, and XIIa Heparin works by potentiating the action of antithrombin III The unfractionated heparin–antithrombin complex produces a 1000-fold increase in antithrombin inhibition of coagulation protein activity compared with antithrombin alone
Antithrombin Antithrombin activity in healthy term neonates is approximately 50% of adult levels, with an increase to the normal range about 6 months after birth Can give FFP or concentrated AT3 to correct antithrombin deficiency
Antithrombin There is about 1 unit of antithrombin in every ml of FFP We currently have recombinant antithrombin available for patients who are refractory to heparin administration and have proven antithrombin deficiency
Antithrombin Consider in patient with heparin resistance ( 60 units/kg/hr of heparin, failure to achieve adequate ACT/anti-Xa level) Side effects of antithrombin administration include bleeding On ECMO, anticipate increased in ACTs with antithrombin administration and need to decrease heparin infusion
Atryn
Atryn (100 - baseline AT activity level) 2.3 X Body Weight (kg) * Recommend recheck of AT level two hours after dose ** This formula is not the same as for the pooled antithrombin product (Thrombate)
Anti-Xa Levels (Heparin Assay) This assay measures unfractionated heparin’s antithrombin-catalyzed inhibition of factor Xa Anti-Xa assay is commonly viewed as a heparin assay despite the fact that it actually represents a measure of unfractionated heparin effect as opposed to a measure of unfractionated heparin concentration
Anti-Xa Levels (Heparin Assay) Our goal anti-Xa level on ECMO is 0.3 to 0.7 IU/mL We can now get anti-Xa levels 24 hours a day, 7 days a week Turn around time for anti-Xa levels is up to 2 hours Currently, using anti-Xa levels to adjust patient goal ACT range
Anticoagulation - Heparin Heparin – “gold standard” for anticoagulation – Not perfect but with wide experience Mechanism of action – Complexes with antithrombin III (AT III) and accelerates its function x 1000 – Requires presence of AT III for its action – Does not affect thrombin formation, only soluble thrombin affected – Does not inhibit thrombin already bound to fibrin – Thrombin formation late in coagulation cascade – Many factors already activated
Anticoagulation - Heparin Small amount of thrombin is continuously formed in circuits despite heparin use Heparin readily reversible with protamine Don’t use protamine on ECMO Heparin itself may cause: – Complement, neutrophil, and monocyte activation – Thrombocytopenia (HIT) – Thrombocytopenia and thrombosis (HITT)
Anticoagulation Heparin Patients respond individually to given dose – Heparin titrated individually for every patient Half-life time 1- 2hr – Affected by renal and hepatic function Excreted in urine – Some amount as unchanged drug
Heparin Dosing Load at cannulation time 100 U/kg (50U/kg if coagulopathic or transthoracic cannulation) – ordered by ICU team with continuous infusion 10–80 U/kg/hr to follow, after ACT 300 seconds Infusion titrated based on hourly ACT’s - Initial targeted ACT 200-220 - Currently, changing target ACT based on anti-Xa level
Heparin dosing Heparin infusion may need to be increased – During platelet infusion – During brisk diuresis Lower ACT’s despite heparin infusion may suggest AT III deficiency
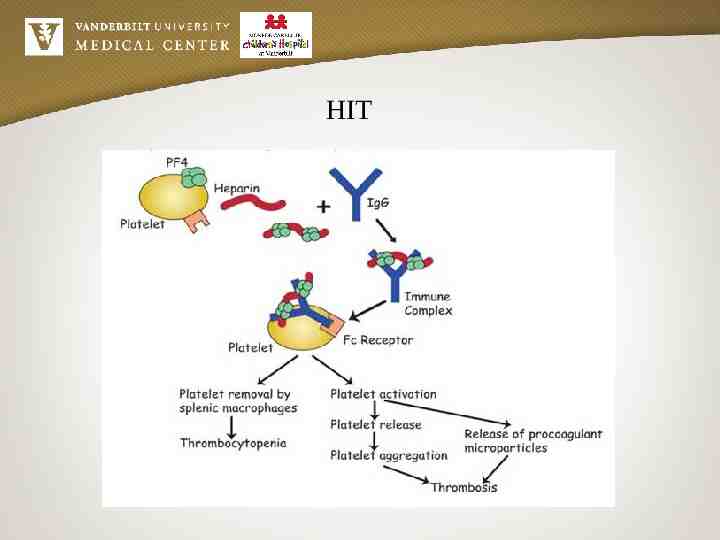
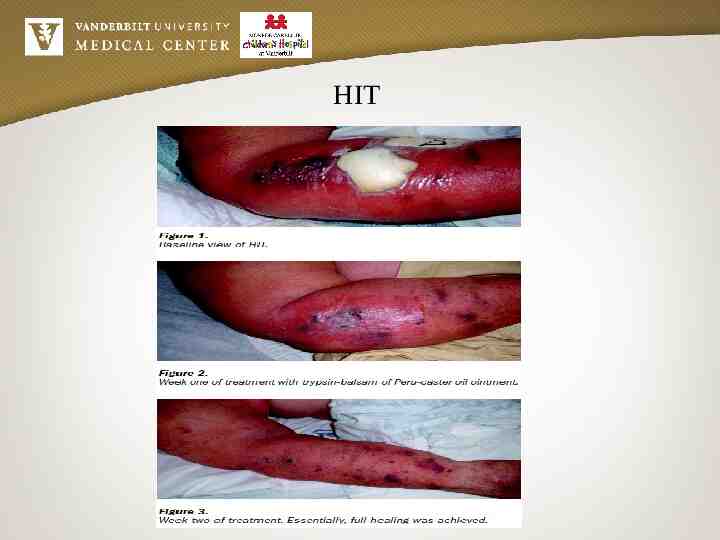
Coagulation HIT Heparin Induced Thrombocytopenia (HIT) usually occurs 4-10 days after initiation of heparin therapy – antibodies to the heparin-platelet factor 4 complex The antibody/antigen complex activates platelets causing further factor 4 release creating a positive feedback loop The thrombocytopenia is rarely severe but patient refractory to platelet transfusion Can lead to thrombosis (HITT)
HIT
Coagulation HIT HIT type 1 is a less severe form of the disease, with mild, early decrease in platelet count that improves even with the ongoing heparin, thrombotic complications generally do not occur HIT type 2 results in a more severe degree of thrombocytopenia, which does not resolve without cessation of heparin therapy and includes the potential for thrombotic complications, both the arterial and venous
Coagulation HIT HIT incidence is highest with unfractionated heparin In most cases, the platelet count decreases 7–14 days after exposure to heparin, but platelet count may fall immediately on re-exposure to heparin If circulating antiheparin IgG antibody present from a previous exposure
Coagulation HIT Antibody (PF4) ELISAs are sensitive but not specific, high false positive rate Functional assays based on in vitro heparin-dependent platelet activation (14C serotonin release, heparin-dependent platelet aggregation, lumiaggregometry) are more specific for clinical HIT Functional assays are less sensitive and often negative or indeterminate in the first 24-48 hours of HIT Both assays usually become negative in about 3 weeks, making it difficult to diagnose previous HIT
HIT
Argatroban Alternative to heparin Direct thrombin inhibitor Goal PTT 65-100 INR may be falsely elevated
Coagulation Circuit DIC Represents a consumptive coagulopathy caused by clot within the circuit Consistently abnormal clotting profile (low plts/fibrinogen) unresponsive to frequent blood product transfusions Increasing D-dimer levels Resolves with a change of circuit
Future Directions for Vanderbilt Study of heparin use, blood product administration, and bleeding/clotting complications since start of coagulation lab protocol Heparin assay protocol specific to ECMO for the bedside specialist Decreasing the other coagulation labs (PTT, ACT)
Future of ECMO Hemostasis More bio-friendly surface circuit materials – Heparin coated – New polymers New anticoagulants – Direct thrombin inhibitors (argatroban, hirudin, bivalirudin) – Nafamostat mesilate – NO in sweep gases – Regional Citrate Anticoagulation
Questions?