EARLY PATIENT MOBILITY February 26, 2020



50 Slides3.97 MB
EARLY PATIENT MOBILITY February 26, 2020
SUBMITTING QUESTIONS Ohio Hospital Association ohiohospitals.org Insert Presentation Title Insert Audience/Group 2/12/23 2
HIIN WEBSITE ohiohospitals.org/HIIN Ohio Hospital Association ohiohospitals.org Insert Presentation Title Insert Audience/Group 2/12/23 3
CONTINUING EDUCATION The link for the evaluation of today’s program is: https:// www.surveymonkey.com/r/CORE-2-26-2020 Please be sure to access the link, complete the evaluation form, and request your certificate. The evaluation process will remain open two weeks following the webcast. Your certificate will be emailed to you when the evaluation process closes after the 2 week process. If you have any questions please contact Dorothy Aldridge ([email protected]) Ohio Hospital Association ohiohospitals.org Insert Presentation Title Insert Audience/Group 2/12/23 4
Early Mobility In The ICU Presented by Scott Tremmel senior PT
Early Mobility In The ICU Cleveland Clinic/ South Pointe Hospital/ ICU Project Leader: Scott Tremmel, PT, Senior Staff Therapist Project Team: Roman Saini, RN, MSN, Nancy Hodge RN, MSN, Jessica Kuczmarski, RN, BSN, Jennifer Williams RN, BSN. Frances Byrne, RN, BSN Project Sponsor: Jacqueline Nowlin, DNP, MBA, RN, NEA-BC Coaches: Anne Spadaro, PT, DPT Manager, Mei Chang, RN, BSN, Quality Coordinator Start Date: 10/1/2019
Objectives Define Mobility Analyze Four Domains Impacted By Hospital Stay Review South Pointe ICU solve project 6 Clicks and nursing Mobility Affect
MOBILITY IS MEDICINE!
Mobility Defined as the ability to move about free and easy The simple tasks we take for granted - Walking Making dinner Visiting friends and loved ones Driving Getting dressed Laughing
Why Does Mobility Matter In The Hospital? 83% of hospital stays are spent lying in bed - .2-21% spend standing or walking (B Kalisch, S Lee and B Dabney, 2013) Decline in walking ability occurs within two days of a hospital stay Up to 3 months after a hospital stay patient can have continue decline in the ability to walk Loss of mobility loss of independence
Four Domains Impacted By Prolonged Hospital Stay A study by (B.Kalish,S. Lee and B. Dabney, 2013) created four domains of impact Physical outcomes - Muscle break down, decline in cardiopulmonary function, skin breakdown, pain, ect . Psychological outcomes - Depression, delirium, anxiety, mood, satisfaction Social outcomes - Quality of life and independence Organizational outcomes - Length of stay and cost
Physical Effects Decline in muscular strength: - Patients lose 1-3% muscle mass daily - 6-40% muscle mass in a week - On average one day of best rest can take 2-3 days of rehab to recover strength Muscle Contractures can develop in 8 hours
Physical effects Cardiopulmonary function breaks down even faster than muscles!
Physical Effects Skin integumentary system breaks down creating pressure ulcers Ulcers commonly develop over areas of bony prominences Cost to treat a stage 2 or greater pressure ulcer in the US: - 70,000 per patient (HIIN)
Physical Effects One of the number one way to prevent a pressure ulcer is through: mobility Pressure relief through positional changes should be occurring every 20-30 minutes
Physiological Effects Delirium - An acute disturbance in mental abilities that results in confused thinking and reduced awareness of the environment - Two subsets: Hyperactive: agitation and aggressive behaviors Hypoactive: lethargy - Can lead to poor clinical outcomes and increasing ICU length of stays (J, Choi 2013) Depression/ Anxiety - Multiple research studies show a range of 13 to over 50% of ICU patients develop some form of depression
Social Effects Loss of independence - Studies show up to 59% loss ability to independently ambulate in the hospital Decrease time spending with friends and family Loss of quality of life Higher change of discharge to Skilled Nursing Facilities
Organizational Prolonged hospital stay - Every hour of length of stay can be up to 100,000 yearly Decrease in hospital admissions due to lack bed availability Cost of bed sores - United States spends approximately 10.2 billion on ulcers a year Increase discharges to Skilled Nursing Facilities - Increases length of stay due to waiting for insurance company precerts - Average stay cost medicare 27,500
Organizational Nursing and caregiver injuries - Greater likely hood of staff injuries can occur due mobilizing patients with hospital acquired weakness - Weaker the patient more likely to require moderate to maximal assistance with transfers - Caregiver injuries lead to shortage in staffing and quality of care provided
“What you do makes a difference, and you have to decide what kind of difference you want to make.” Jane Goodall
A CALL TO ACTION South Pointe hospital Solve Project 2019 MOBILITY IS MEDICINE!
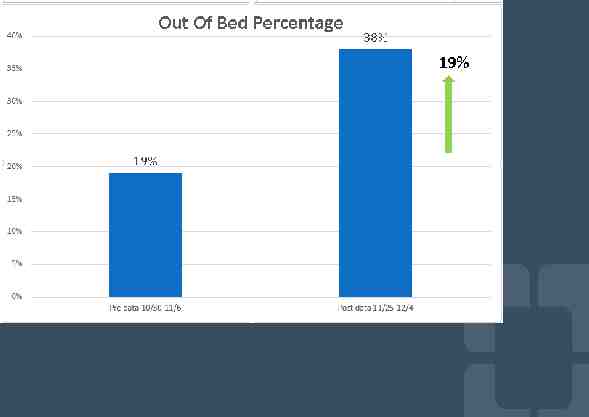
Problem Statement On average, only 38% of SP ICU patients with mobility orders are transferring out of bed with a target of 90%. Aim Statement Increase average percent of patients with mobility orders transferring out of bed from 38% to 90% by end of 1st quarter of 2020.
Expected Benefits South Pointe ICU OKR: Be Responsible Steward to our Length of Stay Resources Decrease ICU and Hospital Length of Stay Reduce Number of Patients Discharged to Skilled Nursing Facilities Decrease Hospital Re-Admission Rate
Expected Benefits South Pointe ICU OKR Zero Harm to the Safety of Patients Decrease Hospital Acquired Illness And Weakness Increase Patient Satisfaction Change The Culture In The ICU Create Best Practice For Patient Mobility
Process Map
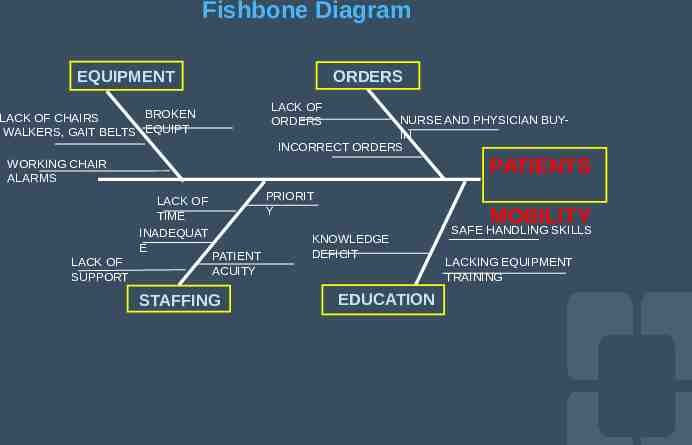
Fishbone Diagram EQUIPMENT ORDERS LACK OF ORDERS BROKEN LACK OF CHAIRS WALKERS, GAIT BELTS EQUIPT NURSE AND PHYSICIAN BUYIN INCORRECT ORDERS PATIENTS WORKING CHAIR ALARMS LACK OF TIME INADEQUAT E LACK OF SUPPORT PRIORIT Y PATIENT ACUITY STAFFING MOBILITY KNOWLEDGE DEFICIT EDUCATION SAFE HANDLING SKILLS LACKING EQUIPMENT TRAINING
Impact vs Effort Chart
Implemented Counter Measures 1. Orders: - Nursing managers daily chart audits for activity orders - Residents placing mobility orders during ICU morning rounds 2. Education: - Morning huddle education by nursing staff and Physical Therapist - Educational posters 3. Equipment: - Walker and Chair inventory 4. Staffing - PT rounding in AM and PM to assist with transfers
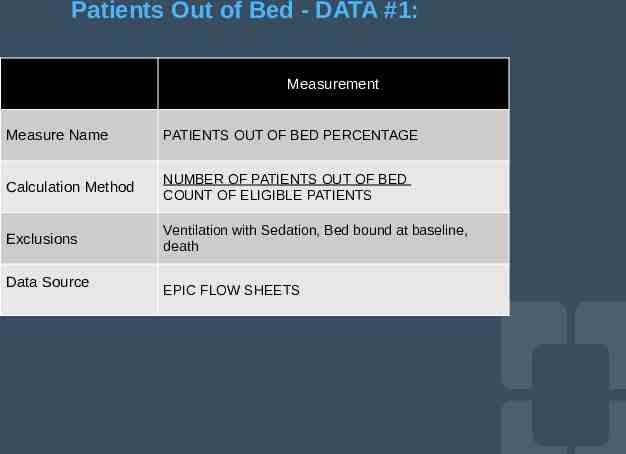
Patients Out of Bed - DATA #1: Measurement Measure Name PATIENTS OUT OF BED PERCENTAGE Calculation Method NUMBER OF PATIENTS OUT OF BED COUNT OF ELIGIBLE PATIENTS Exclusions Ventilation with Sedation, Bed bound at baseline, death Data Source EPIC FLOW SHEETS
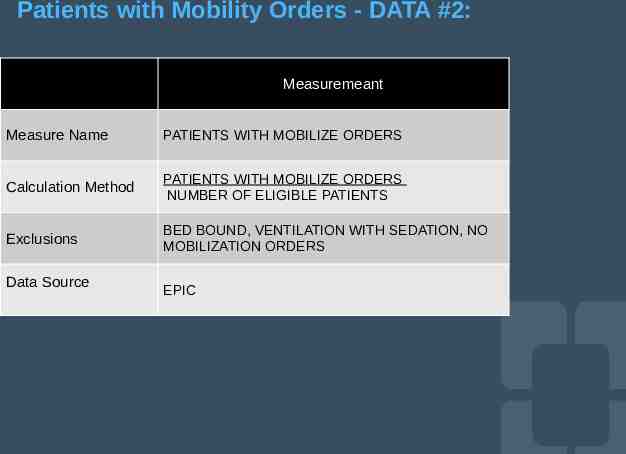
Patients with Mobility Orders - DATA #2: Measuremeant Measure Name PATIENTS WITH MOBILIZE ORDERS Calculation Method PATIENTS WITH MOBILIZE ORDERS NUMBER OF ELIGIBLE PATIENTS Exclusions BED BOUND, VENTILATION WITH SEDATION, NO MOBILIZATION ORDERS Data Source EPIC
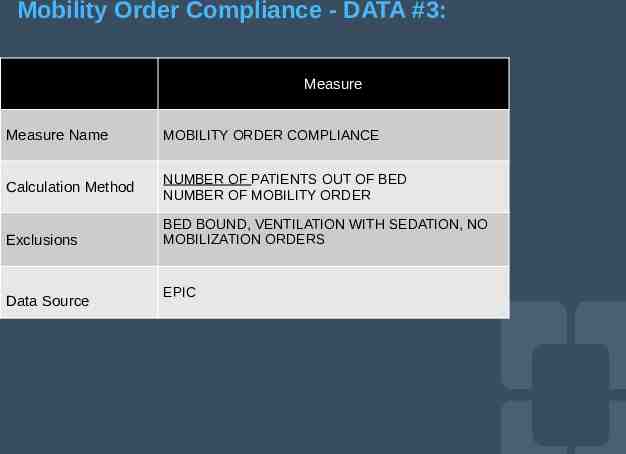
Mobility Order Compliance - DATA #3: Measure Measure Name MOBILITY ORDER COMPLIANCE Calculation Method NUMBER OF PATIENTS OUT OF BED NUMBER OF MOBILITY ORDER Exclusions Data Source BED BOUND, VENTILATION WITH SEDATION, NO MOBILIZATION ORDERS EPIC
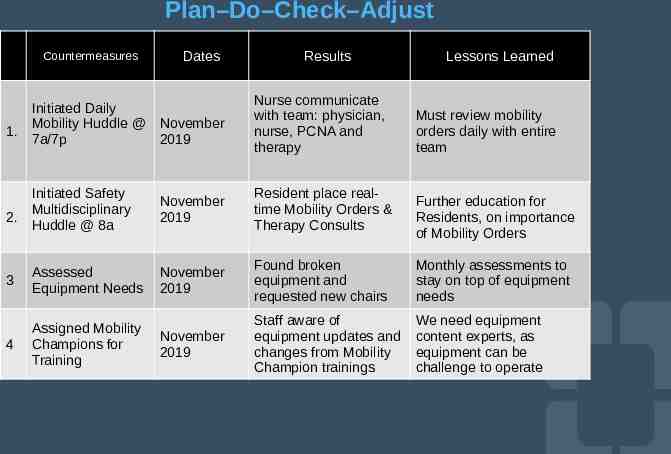
Plan–Do–Check–Adjust Countermeasures Dates Results Lessons Learned Initiated Daily Mobility Huddle @ November 7a/7p 2019 Nurse communicate with team: physician, nurse, PCNA and therapy Initiated Safety Multidisciplinary Huddle @ 8a November 2019 Resident place realtime Mobility Orders & Therapy Consults 3 Assessed Equipment Needs November 2019 Found broken equipment and requested new chairs Monthly assessments to stay on top of equipment needs 4 Assigned Mobility Champions for Training November 2019 Staff aware of equipment updates and changes from Mobility Champion trainings We need equipment content experts, as equipment can be challenge to operate 1. 2. Must review mobility orders daily with entire team Further education for Residents, on importance of Mobility Orders
Takeaways Mobility is Medicine and beneficial for optimal patient care.
Takeaways All disciplinary team members are necessary to drive the results. Activity orders are important and need to be followed appropriately. Proper equipment and training is required to mobilize patients. Ongoing training for nurses, therapist, physicians, PCNA’s is needed for sustainability.
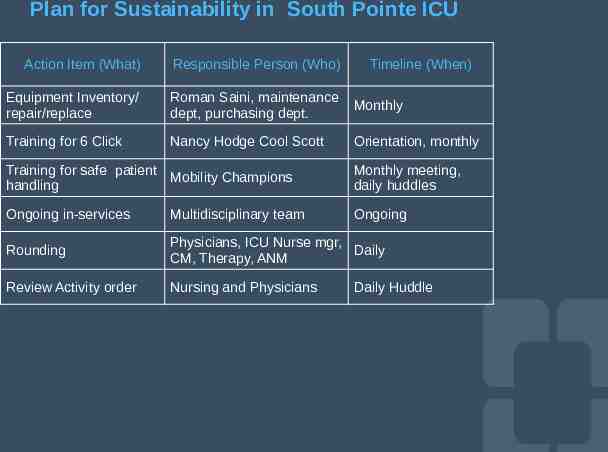
Plan for Sustainability in South Pointe ICU Action Item (What) Responsible Person (Who) Timeline (When) Equipment Inventory/ repair/replace Roman Saini, maintenance dept, purchasing dept. Monthly Training for 6 Click Nancy Hodge Cool Scott Orientation, monthly Training for safe patient Mobility Champions handling Monthly meeting, daily huddles Ongoing in-services Multidisciplinary team Ongoing Rounding Physicians, ICU Nurse mgr, Daily CM, Therapy, ANM Review Activity order Nursing and Physicians Daily Huddle
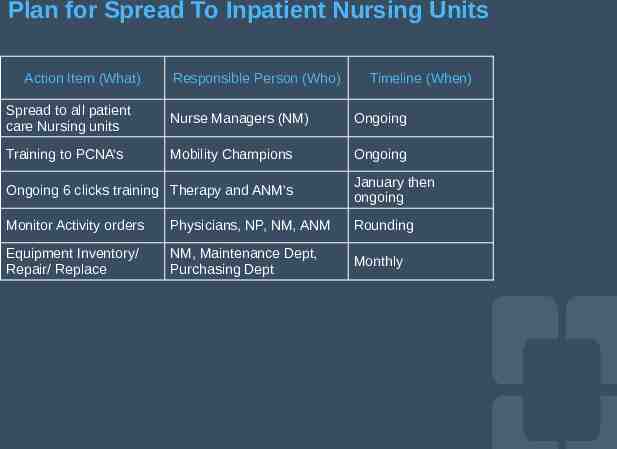
Plan for Spread To Inpatient Nursing Units Action Item (What) Responsible Person (Who) Timeline (When) Spread to all patient care Nursing units Nurse Managers (NM) Ongoing Training to PCNA’s Mobility Champions Ongoing Ongoing 6 clicks training Therapy and ANM’s January then ongoing Monitor Activity orders Physicians, NP, NM, ANM Rounding Equipment Inventory/ Repair/ Replace NM, Maintenance Dept, Purchasing Dept Monthly
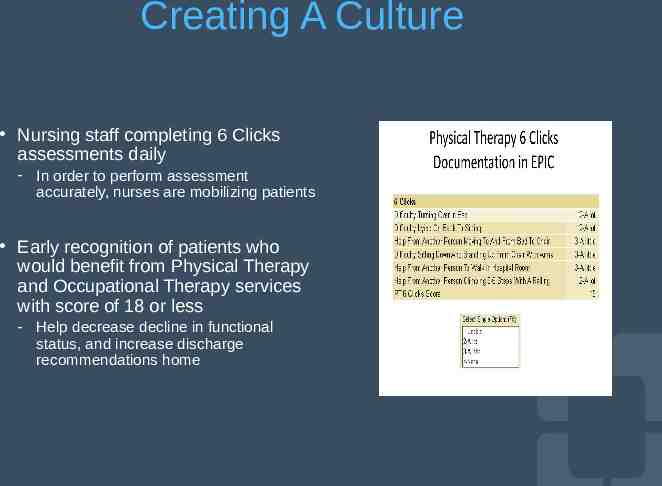
Creating A Culture Nursing staff completing 6 Clicks assessments daily - In order to perform assessment accurately, nurses are mobilizing patients Early recognition of patients who would benefit from Physical Therapy and Occupational Therapy services with score of 18 or less - Help decrease decline in functional status, and increase discharge recommendations home
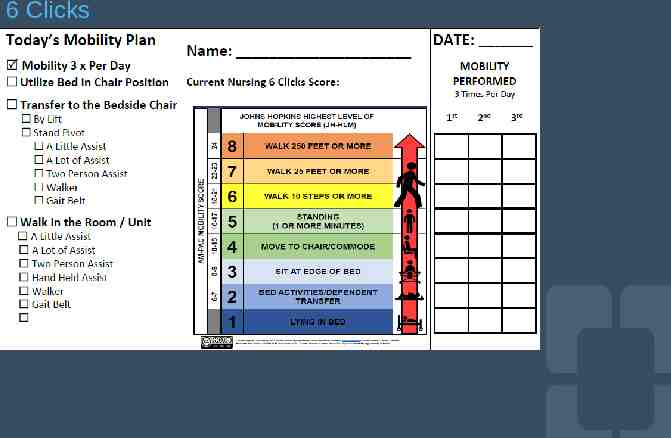
6 Clicks
The Mobility Affect Early mobilization can help prevent muscle wasting Promotes cardiovascular function Relieves pressure on the skin avoiding sore Improves cognition and awareness of surroundings Helps improve mental strength and decrease depression More patients are able to return home Decrease in length of stay Greater satisfaction scores Finally decreasing functional decline, can lead to less caregiver injury from patient imbalance
The Choice is Yours! Attributing the Responsibility for ambulating patients: A qualitative study - Nurses can be broken down into two groups: Those who claimed ambulation of patients within their responsibility Resulting in actions related to collaborating with Physical Therapy, determining the appropriateness of activity orders, diminishing the risk and adjusting to recourses available Those who attributed the responsibility deferred decisions about initiating ambulation to either Physical Therapy or medicine Resulting in actions related to waiting, which involved, waiting for Physical Therapy clearance, physician orders, risks ti decrease, and resources to improve before ambulating (B Doherty-King and B Bowers, 2013)
“The way to get started is to quite talking and begin doing!” Walt Disney
References Barbara Doherty-King and Barbara J. Bowers. Attributing the Responsibility for Ambulating Patients: A qualitative Study.Int J Nurs Stud. 2013 September: 1240-1246 Beatrice J Kalisch, Soohe Lee and Beverly W Dabney. Outcomes of Inpatient Mobilization: a Literature Review. J of Clinical Nurs. 2013,23:1486-1501 Yi Tian Wang, Terry P Haines, Paul Ritchies, Craig Walker, Teir A Ansell, Danielle T Ryan, Phaik-Sim Lim, Sanjiv Vij, Rebecca Acs, Nigel Fealy and Elizabeth Skinner. Early Mobilization on Continuous Renal Replacement Therapy is Safe and May Improve Filter Life. Critical Care. 2014, 18:R161 Jun Gwon Cho. Delirium in the Intensive Care Unit. Korean J Anesthesiol. 2013 Sep; 65(3): 195–202. www.hret-hiin.org
SUBMITTING QUESTIONS Ohio Hospital Association ohiohospitals.org Insert Presentation Title Insert Audience/Group 2/12/23 49
OHA collaborates with member hospitals and health systems to ensure a healthy Ohio James Guliano, MSN, RN-BC, FACHE Rosalie Weakland Vice President, Quality Programs Senior Director, Quality Programs [email protected] [email protected] — Ohio Hospital Association 155 E. Broad St., Suite 301 Columbus, OH 43215-3640 T 614-221-7614 ohiohospitals.org — HelpingOhioHospitals @OhioHospitals www.youtube.com/user/OHA1915