Diversity & Cultural Competence in Respiratory Care



















52 Slides2.58 MB
Diversity & Cultural Competence in Respiratory Care
Objectives Identify how the beliefs, attitudes and behaviors of major American cultural groups impact public health. Create heightened appreciation for the influence of cultural competency in health care. Identify strategies for enhancing cultural competency in respiratory care.
WHAT IS CULTURAL COMPETENCE?
Basic Diversity Terminology Culture: An integrated pattern of human behavior that includes thoughts, communications, languages, practices, beliefs, values, customs, courtesies, rituals, manners of interacting, roles, relationships and expected behaviors of a racial, ethnic, religious or social group.
Culture Defined Broadly Term culture inclusive of: – – – – – – Race Language Ethnicity Gender Sexual Orientation Shared Experiences (i.e. poverty, mental illness, addiction, homelessness, etc.)
What Culture is Not: Culture is not: – – Race Stereotypic generalizations about the behaviors, emotions and values of a group of people. – A laundry list of values behaviors and facts related to a group of people. – Rigid or static categorizations of people without a deep and fundamental awareness of their differences. – Superficial adoption of customs, language, dress or behavior in a patronizing manner. “What is Cultural Competence?”, Family Resource Coalition Report, Fall/Winter 1995-96
Basic Terminology Cultural awareness: Being cognizant, observant and conscious of similarities and differences among cultural groups Cultural sensitivity: Understanding the needs and emotions of your own culture and the culture of others. Cultural Competence: Has many definitions!
Definitions of Cultural Competence Cross et al, 1989 Cultural competence is a set of congruent behaviors, attitudes, and policies that come together in a system, agency or among professionals and enable that system, agency or those professions to work effectively in cross-cultural situations.
Definitions of Cultural Competence Denboba, MCHB, 1993 a set of values, behaviors, attitudes, and practices within a system, organization, program or among individuals and which enables them to work effectively cross culturally. the ability to honor and respect the beliefs, language, interpersonal styles and behaviors of individuals and families receiving services, as well as staff who are providing such services.
Definitions of Cultural Competence Health Resources and Services Administration, Bureau of Primary Health Care Cultural and linguistic competence is a set of congruent behaviors, attitudes and policies that come together in a system, agency or among professionals that enables effective work in crosscultural situations. "Culture" refers to integrated patterns of human behavior that include the language, thoughts, communications, actions, customs, beliefs, values, and institutions of racial, ethnic, religious or social groups. "Competence" implies having the capacity to function effectively as an individual and an organization within the context of the cultural beliefs, behaviors and needs presented by consumers and their communities
Cultural Competence Within the Health Care System Requires: Culturally Competent Care: Administered with sensitivity for a patients culture and health-related beliefs. Culturally Competent Staff: That reflect the ethnic communities they serve with understanding and respect for the beliefs, attitudes, interpersonal styles and healthrelated beliefs of their patients. Organizational Management: Who develop policy, procedures and processes the assure uniform patient care.
Changing National Demographics Changing demographics result in an increased need to medical delivery responsive to multicultural populations: Population Size and Composition: 2003 Approximately 33.5 million foreign-born people live in the United States. The foreign born represent 11.7 percent of the U.S. population. Source: US Census Bureau, Current Population Survey, Annual Social and Economic Supplement, 2003
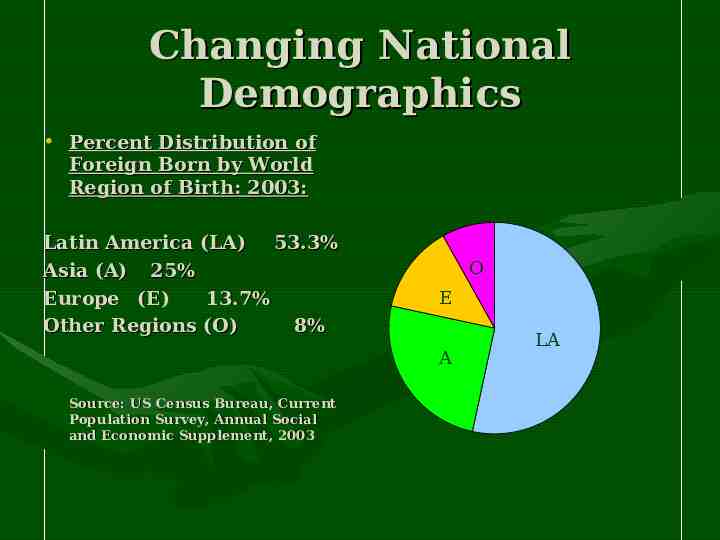
Changing National Demographics Percent Distribution of Foreign Born by World Region of Birth: 2003: Latin America (LA) 53.3% Asia (A) 25% Europe (E) 13.7% Other Regions (O) 8% O E A Source: US Census Bureau, Current Population Survey, Annual Social and Economic Supplement, 2003 LA
Different Customs, Beliefs and Practices AMERICAN/WESTERN CULTURES Health is absence of Disease Seeks traditional health care providers (i.e. physicians, nurses, surgeons, psychiatrists) Seeks medical system to prevent and treat illness Values independence and freedom NONWESTERN CULTURES Health is a state of harmony within body, mind, spirit Seeks alternative medical practitioners (i.e. herbalists, shamans, midwives etc.) Seeks medical system when in acute stage of illness Values interdependence with family and community Future oriented Present oriented: here and now Gestures have universal meaning Gestures have taboo meanings, depending on culture Individual interests are Individual interests are Physician Toolkit: To Implement Cross-Cultural Clinical Practice Guidelines for subordinate to family needs Medicaid Practitioners, March, 2004 valued and encouraged
Why be Culturally Competent? Because many cultures populate our country: – Culture inclusive of many factors – Changing national demographics. – Vast array of customs, beliefs, practices Because it’s the law.
Why be Culturally Competent? Because It’s the Law: – The Civil Right’s Act of 1964: Title VI “No person in the United States shall, on the grounds of race, color or national-origin, be excluded from participation in, denied the benefit of, or be subjected to discrimination under any program or activity receiving federal financial assistance.”
It’s the Law Emergency Medical Treatment and Active Labor Act : Also known as the Patient Antidumping Act, requires hospitals that participate in the Medicare program that have emergency departments to treat all patients (including women in labor) in an emergency without regard to their ability to pay.
It’s the Law Medicaid : Medicaid regulations require Medicaid providers and participating agencies, including long-term care facilities, to render culturally and linguistically appropriate services.
It’s the Law Medicare Medicare addresses linguistic access in its reimbursement and outreach education policies. “Medicare providers are encouraged to make bilingual services available to patients wherever the services are necessary to adequately serve a multilingual populations.”
Importance of Cultural Competence Cultural Competence is necessary to improve the health care outcomes of a culturally diverse population of patients who utilize the health care system.
Health Care Disparities Research indicates that clinical encounters between culturally insensitive health care practitioners and patients from different cultural backgrounds can contribute to disparities and barriers to appropriate health care.
Health Care Disparities Disparities in health care delivery has been documented among: – – – – – – African Americans Latino/Hispanics Native Americans Asians Alaskans Pacific Islanders
Health Care Disparities In the U.S., ethnic minority populations lag behind the European population on a number of key health indicators including: – – – – Health care coverage Access to health care Life expectancy Acute and chronic disease states
Health Care Disparities Common barriers to providing culturally sensitive health care include: – Underestimation of need for service – Lack of appreciation for cultural belief differences related to illness, suffering, and dying – Language and other communication barriers
Health Care Disparities Culturally competent health care guidelines will help eliminate these disparities.
Key Components of Culturally Appropriate Care Include: Attitude Hiring and Training Skills Culturally Diverse Health System
Attitude Culturally Biased Health Care Patients from other races and socio-economic status tend to be viewed more negatively by physicians (VanRyn and Burke, 2000) Hispanics and Blacks are less likely to receive major therapeutic and diagnostic procedures for their conditions ( VanRyn and Burke, 2000) Vietnamese, Hispanics and Blacks have higher mortality rates for cancer and studies indicate that physicians manage cancer different based on race ( Bach et al, 1999: King and Brunetta, 1999)
Attitude Culturally Biased Health Care: A patient’s race and gender have been shown to influence a physicians decision to refer for cardiac catherization. (Schulman et al, 1999) Physicians fail to recognize the presence of pain in patients who are culturally different resulting in under medication. (Todd et al, 1993)
Attitude Cultural competence requires willingness to adapt to the needs of patients and their family members, and to meet those needs in an objective, non-judgmental way including – – – – Ability to demonstrate empathy Ability to value diversity The capacity for cultural self assessment Awareness of the dynamics that exist when cultures interact – A clinical demeanor based on an understanding of cultural diversity
Hiring and Training for Cultural Competence Hire a culturally diverse work force. Develop a comprehensive training curriculum in the elements of cultural competence. Mandate training in language, medical interpretation and cultural competence for all employees as required by their position. Allocate the budget and time for employee orientation, training and up-dates in the area of cultural competence
Skills Cultural competence requires behaviors that exemplify appropriate interactions between health care professionals and their patients in the areas of: – Patient cultural assessment – Treatment planning and adherence – Patient education and communication – Clinical decision making
SKILLS Patient Cultural Assessment: the need to assess cultural, environmental and socioeconomic factors as part of diagnostic procedures. – Cultural: Race, family structure, gender roles, religion and spirituality, dietary habits and time/space orientation. – Social: Support networks, socioeconomic status, community resources, literacy level and lifestyle behaviors. – Environment: Aculturalization, knowledge of U.S health care system, political history, racism and discrimination and geographic access.
SKILLS Models for patient cultural assessment: – LEARN model (Berlin and Fowke’s): (L) – Listening to the patients perspective (E) – Explaining and sharing one’s own perspective (A) – Acknowledging differences and similarities between the two perspectives. (R) – Recommend a treatment plan (N) – Negotiating a mutually agreed-on treatment plan
SKILLS Models for patient cultural assessment: – Patient Explanatory Model (Klienman et al) Elicitation techniques for gaining information from patient and/or family members about onset, treatment and prognosis: What do you call your problem? What name does it have? What do you think caused your problem? What is your sickness doing to you? What problems has it caused you? Will it last a short or long time? What type of treatment do you think you should get? What do you hope to get from the treatment?
TREATMENT PLANNING AND ASSESSMENT Factors affecting treatment planning: – Cultural health beliefs Traditional/folk medicine practiced Religious practices Patients views about health, medications and health care establishment – Role of family Family member designated as key decision maker Family members responsible for giving and monitoring care Extended family members to be included in care planning
TREATMENT PLANNING AND ASSESSMENT Factors affecting treatment planning: – Socioeconomic factors Ability to pay for treatment over time Limited resources may lead to skipping or sharing medications with other family members – Environmental factors Patients work schedule can result in missed appointments Lack of transportation presents barriers to keeping appointments Exposure to environmental toxins ( i.e. pollution, allergens, roaches, etc.) can decease the effectiveness of therapy Physician Toolkit: To Implement Cross-Cultural Clinical Practice Guidelines for Medicaid Practitioners, March, 2004
TREATMENT PLANNING AND ASSESSMENT Negotiation of treatment plans: – The patient and the healthcare provider must acknowledge their differences about the treatment plan/methods and come to a mutually-agreeable but beneficial alternative. – Process of negotiation involves: Relationship building Problem clarification Agenda setting Assessment Follow-up care management
Patient Communication/Education Barriers to effective communication: – Lack of awareness of patient expectations – Devaluing the patient or the patients’ family health care views – Language barriers – Cultural norms/customs for interpersonal communication – Patient feeling rushed – Physician biases Collins et all, 2002; IOM, 2003:Rivadeneyra et al., 2000
Promote Effective Communication Translation: When written words in one language are translated into another. Patient materials must be developed and written in the clients language. Interpretation: Conversation between two speaker is translated from one language to another including sign language. This is usually performed by a third party. Medical Interpretation: Goes beyond routine interpretation with emphasis placed on the ability to interpret for the provider and the patient within a medical context
Patient Communication/Education Suggested strategies for effective crosscultural communication: – Use open ended questions – Collect information via conversation rather than intensive questioning. – Do not interrupt the patient – Communicate in an unhurried manner – Allow the patient time to ask questions – Speak in a normal tone – Explain medical terms in simple language – Use validating techniques to assure the patient you are listening.
Patient Communication/Education Suggestions for non-verbal cross-cultural communication: Speak directly to the patient. Understand that lack of eye contact may not imply lack if interest. Limit the use of gestures. Be aware of the patients’ cultural norms for appropriate distance. Social touching of the patient may be unacceptable. Slouching or exposing the sole of the foot can be viewed as unacceptable. Use interpreters when needed.
Patient Communication/Education Patient education to help in understanding the nature and conditions of their illness and changing risky behaviors: – Consider literacy and education level of the patient – Overcome language barriers through the use of interpreters – Incorporate concepts familiar to patient views related to health values, beliefs and practices. Betancourt et al. 1999; Buchwald et al.,1993, Flores, 2000
Clinical Decision Making Culturally sensitive clinical decision making must transcend: – The clinicians preconceived assumptions about the patient and the cause of their illness. – Professional norms, behaviors and training that distance the clinician from the patient and their individual needs. – The complex health care system and institutional operations that promote cost control, clinical productivity and workforce competence over patient preferences and individual needs.
Goals of a Culturally Diverse Health System To value the diverse cultural beliefs of all clients. To promote effective communication between providers and the diverse community of interest they serve. To hire and train for cultural competence with the same seriousness as applied to other essential clinical skills. To institutionalize cultural competence
Institutionalize Cultural Competence Integrate cultural competence into the strategic planning at all levels Include funding for culturally diverse staffing as well as training and other essential activities. Make cultural competence a criterion for employee evaluation. Involve your community of interest in the process of defining and addressing health service needs.
Culturally Competent Health Care is Effective More complete and specific information gathering is provided for the provider resulting in more accurate diagnosis. Treatment plans supported by the family are developed which increase patient compliance. There is a greater use of health services by ethnic populations and reduced delays in seeking care. Communication between healthcare provides and patients is enhanced. The compatibility between Western and traditional health practices is enhanced.
References Cross, T., Bazron, B., Dennis, K., & Isaacs, M., (1989). Towards A Culturally Competent System of Care, Volume I. Washington, DC: Georgetown University Child Development Center, CASSP Technical Assistance Center. Denboba, D., U.S. Department of Health and Human Services, Health Services and Resources Administration (1993). MCHB/DSCSHCN Guidance for Competitive Applications, Maternal and Child Health Improvement Projects for Children with Special Health Care Needs. Census Bureau’s Web site: http://www.census.gov, Foreign-Born Population Data Paulson and Dekker,, Healthcare Disparities in Pain Management, J Am Osteopath Assoc 2005;105:S14-S17. James et al., Association of Race/Ethnicity with Emergency Department Wait Times, Pediatrics 2005;115:e310-e315 Kagawa-Singer and Blackhall, Negotiating Cross-Cultural Issues at the End of Life: "You Got to Go Where He Lives, JAMA 2001;286:2993-3001
References Achieving Cultural Competence: A Guidebook for Providers of Services to Older Americans and Their Families: www.aoa.gov/prof/adddiv/ culture/CC-guidebook.pdf “Health Care RX: Access for ALL”,The Presidents Initiative on Race, U.S. Department on Health and Human Services, Health Resources and Service Administration, 1999, P.17-18.