Delivering Screening, Brief Intervention, and Referral to Treatment to




24 Slides5.12 MB
Delivering Screening, Brief Intervention, and Referral to Treatment to Mitigate High-Risk Substance Use in STI Clinical Settings
Presenter Introduction (Note: Slide serves as a placeholder for presenter(s) who wish to include their picture and any introductory information.) First Name and Last Name Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat.
SBIRT Training Overview This training provides an overview of the Screening, Brief Intervention, and Referral to Treatment (SBIRT) intervention, which motivates clients seeking STI services who are engaged in high-risk substance use (HRSU) to pursue HRSU treatment and care services. The following presentation addresses: What is HRSU? What is SBIRT? Evidence Supporting Use of SBIRT to Address HRSU in STI Clinics HRSU and STIs: A Syndemic SBIRT Logistics SBIRT for HRSU: Client Populations and Enrollment Criteria Screenings Promoting the Intervention Educational Materials for Clients Staffing Electronic Health Record (EHR) System SBIRT for HRSU: Intervention Steps Questions and Answers
What is HRSU? High-risk substance use (HRSU) refers to: Use of illicit drugs Non-medical use of prescription drugs Note: focus is on substances that pose a high-risk for negative health outcomes (see below). Does not include the use of alcohol or marijuana. Possible impacts of HRSU: Drug dependence, substance use disorders, and non-fatal and fatal overdoses HIV, viral hepatitis, and other infections or wounds, primarily associated with injection drug use Disinhibition encouraging unprotected sex and needle-sharing, which can drive the spread of STIs and other diseases, including HIV and viral hepatitis. 1,2 Substance use disorder and HRSU rates are often higher among STI clinic clients than the general population.
What is SBIRT? SBIRT for HRSU is a brief behavioral intervention that identifies clients engaged in HRSU through evidence-based screening; offers motivational interviewing to help clients set goals to engage in specific health services; and provides encouragement, referral, and a warm handoff to treatment and care. SBIRT steps include the following: Screening Brief Intervention Referral to Treatment Identifying/assessing the degree of substance use and identifying the appropriate level of treatment among clients; Increasing awareness of substance use among clients, motivating behavior change; and Connecting clients requiring additional services to care.
Evidence Supporting Use of SBIRT to Address HRSU in STI Clinics SBIRT was initially developed to help connect people engaged in alcohol use to treatment. SBIRT has been applied in other clinical settings, including the early identification and intervention for those engaged in substance use who seek services in STI clinics. One 2007 study with New York City STI clinics found that the SBIRT model successfully connected patients with substance use treatment, resulting in improvements in their substance use disorder and mental health, and reduced their condomless sexual contact.4 The Addressing High-Risk Substance Use through STI Clinics: Strengthening Connections to Treatment and Behavioral Health Services project demonstrated the use of the SBIRT intervention to motivate and connect people seeking STI services who are engaged in HRSU with HRSU treatment and care services. 5
Evidence Supporting Use of SBIRT to Address HRSU in STI Clinics Persons engaged in HRSU at STI clinics report higher rates of: Condomless sex Multiple partners STI diagnoses6 Specific population factors to consider: While men who have sex with men (MSM) have a higher burden of STIs and HRSU than the general population, 7,8,9 increases in STIs and HRSU have been reported among heterosexuals and women as well.10,11,12
Evidence Supporting Use of SBIRT to Address HRSU in STI Clinics Social Determinants of HRSU include: Poverty Homelessness Housing instability Lack of adequate insurance coverage and health care Limited educational attainment13,14,15,16 These determinants also drive additional risk factors for HRSU and STIs: Engagement with the legal system Anonymous sex Sex in exchange for resources, including drugs and money 17,18,19
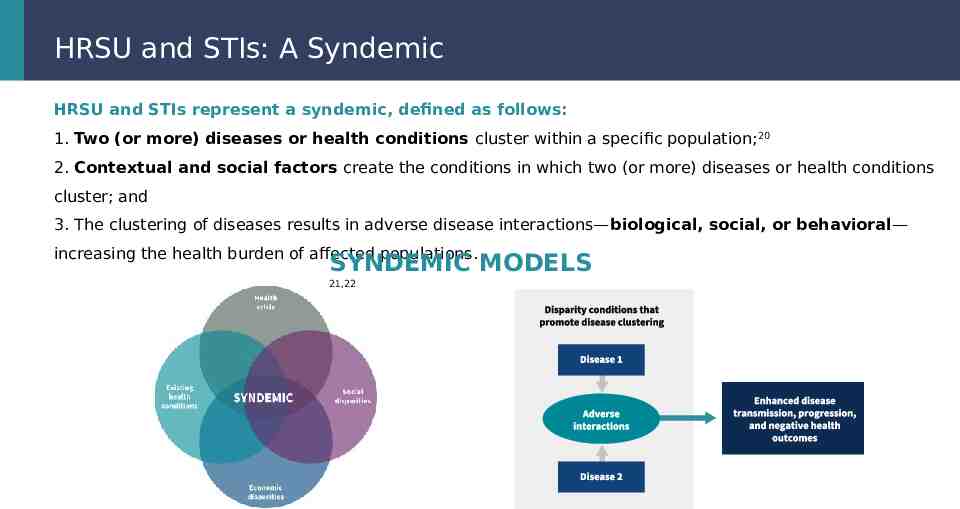
HRSU and STIs: A Syndemic HRSU and STIs represent a syndemic, defined as follows: 1. Two (or more) diseases or health conditions cluster within a specific population;20 2. Contextual and social factors create the conditions in which two (or more) diseases or health conditions cluster; and 3. The clustering of diseases results in adverse disease interactions—biological, social, or behavioral— increasing the health burden of affected populations. SYNDEMIC MODELS 21,22
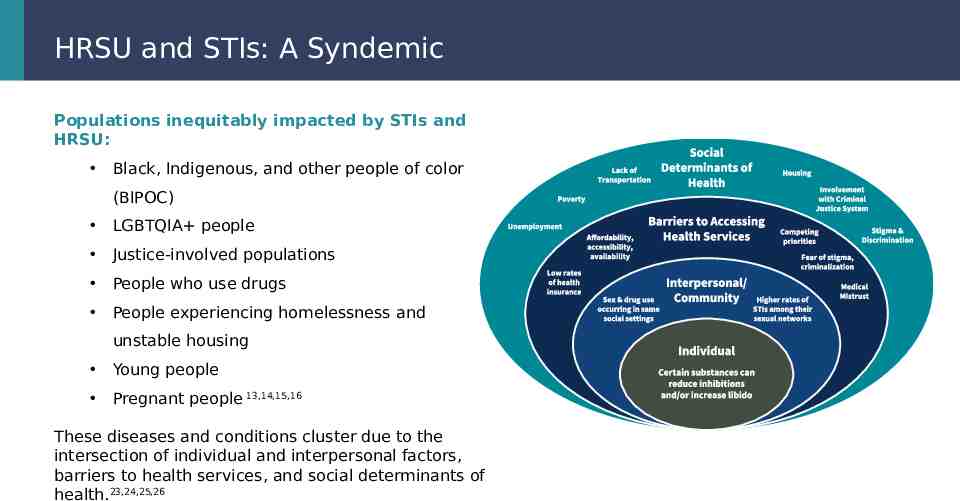
HRSU and STIs: A Syndemic Populations inequitably impacted by STIs and HRSU: Black, Indigenous, and other people of color (BIPOC) LGBTQIA people Justice-involved populations People who use drugs People experiencing homelessness and unstable housing Young people Pregnant people 13,14,15,16 These diseases and conditions cluster due to the intersection of individual and interpersonal factors, barriers to health services, and social determinants of health.23,24,25,26
SBIRT Logistics STI clinics present a unique opportunity to reach people engaged in HRSU and connect them with potentially life-saving treatment and care. Components integral to implementing SBIRT for HRSU in STI clinical settings include: Client Populations and Enrollment Criteria Intervention Promotion Educational Materials for Clients Staffing Electronic Health Record (EHR) System
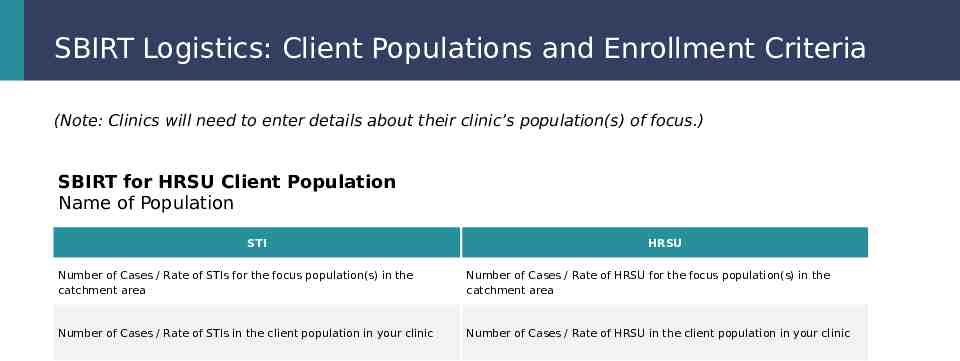
SBIRT Logistics: Client Populations and Enrollment Criteria (Note: Clinics will need to enter details about their clinic’s population(s) of focus.) SBIRT for HRSU Client Population Name of Population STI HRSU Number of Cases / Rate of STIs for the focus population(s) in the catchment area Number of Cases / Rate of HRSU for the focus population(s) in the catchment area Number of Cases / Rate of STIs in the client population in your clinic Number of Cases / Rate of HRSU in the client population in your clinic
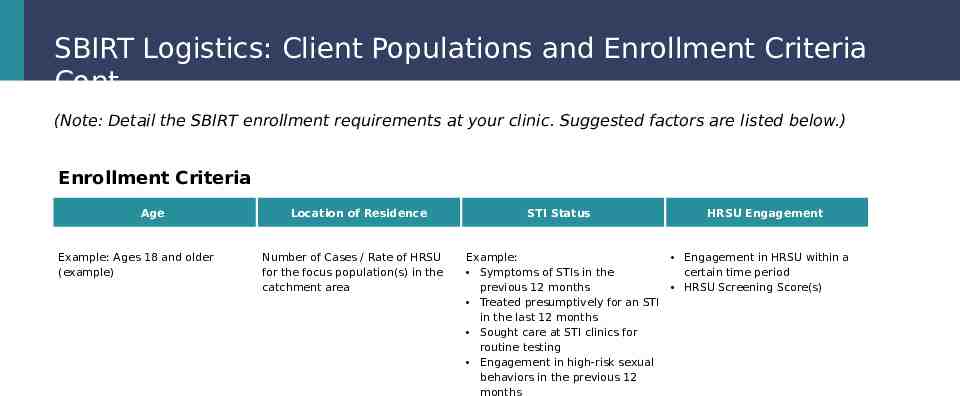
SBIRT Logistics: Client Populations and Enrollment Criteria Cont. (Note: Detail the SBIRT enrollment requirements at your clinic. Suggested factors are listed below.) Enrollment Criteria Age Example: Ages 18 and older (example) Location of Residence Number of Cases / Rate of HRSU for the focus population(s) in the catchment area STI Status Example: Symptoms of STIs in the previous 12 months Treated presumptively for an STI in the last 12 months Sought care at STI clinics for routine testing Engagement in high-risk sexual behaviors in the previous 12 months HRSU Engagement Engagement in HRSU within a certain time period HRSU Screening Score(s)
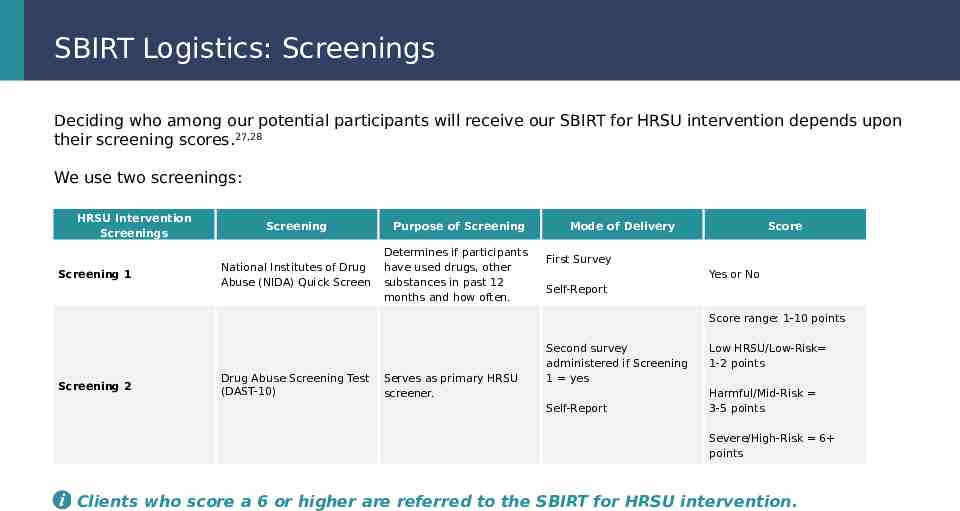
SBIRT Logistics: Screenings Deciding who among our potential participants will receive our SBIRT for HRSU intervention depends upon their screening scores.27,28 We use two screenings: HRSU Intervention Screenings Screening 1 Screening National Institutes of Drug Abuse (NIDA) Quick Screen Purpose of Screening Determines if participants have used drugs, other substances in past 12 months and how often. Mode of Delivery Score First Survey Yes or No Self-Report Score range: 1-10 points Screening 2 Drug Abuse Screening Test (DAST-10) Serves as primary HRSU screener. Second survey administered if Screening 1 yes Self-Report Low HRSU/Low-Risk 1-2 points Harmful/Mid-Risk 3-5 points Severe/High-Risk 6 points Clients who score a 6 or higher are referred to the SBIRT for HRSU intervention.
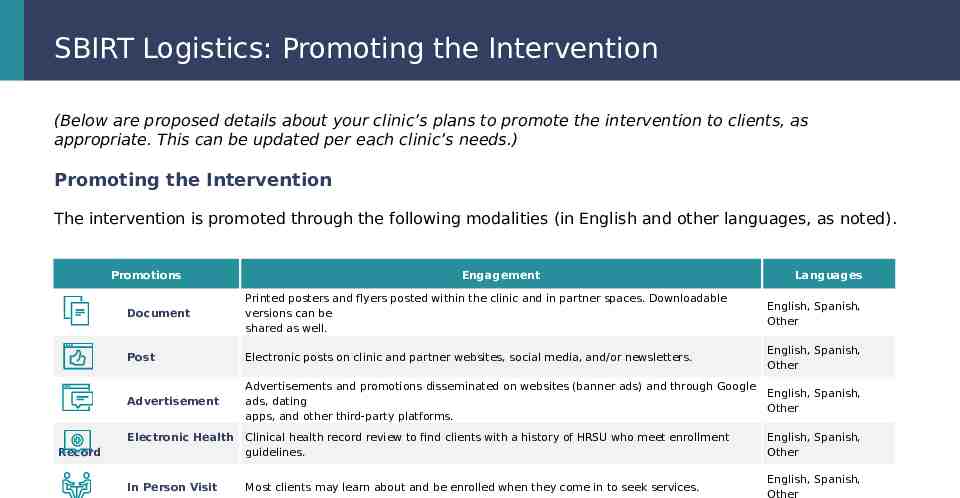
SBIRT Logistics: Promoting the Intervention (Below are proposed details about your clinic’s plans to promote the intervention to clients, as appropriate. This can be updated per each clinic’s needs.) Promoting the Intervention The intervention is promoted through the following modalities (in English and other languages, as noted). Promotions Engagement Languages Document Printed posters and flyers posted within the clinic and in partner spaces. Downloadable versions can be shared as well. English, Spanish, Other Post Electronic posts on clinic and partner websites, social media, and/or newsletters. English, Spanish, Other Advertisement Advertisements and promotions disseminated on websites (banner ads) and through Google ads, dating apps, and other third-party platforms. English, Spanish, Other Electronic Health Clinical health record review to find clients with a history of HRSU who meet enrollment guidelines. English, Spanish, Other In Person Visit Most clients may learn about and be enrolled when they come in to seek services. English, Spanish, Other Record
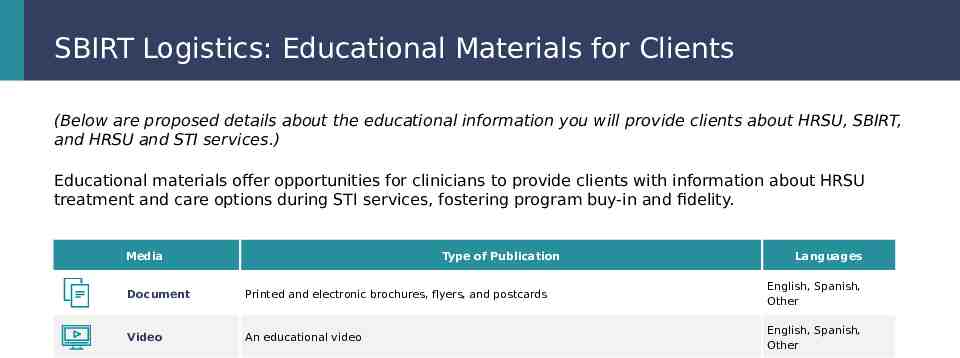
SBIRT Logistics: Educational Materials for Clients (Below are proposed details about the educational information you will provide clients about HRSU, SBIRT, and HRSU and STI services.) Educational materials offer opportunities for clinicians to provide clients with information about HRSU treatment and care options during STI services, fostering program buy-in and fidelity. Media Type of Publication Languages Document Printed and electronic brochures, flyers, and postcards English, Spanish, Other Video An educational video English, Spanish, Other
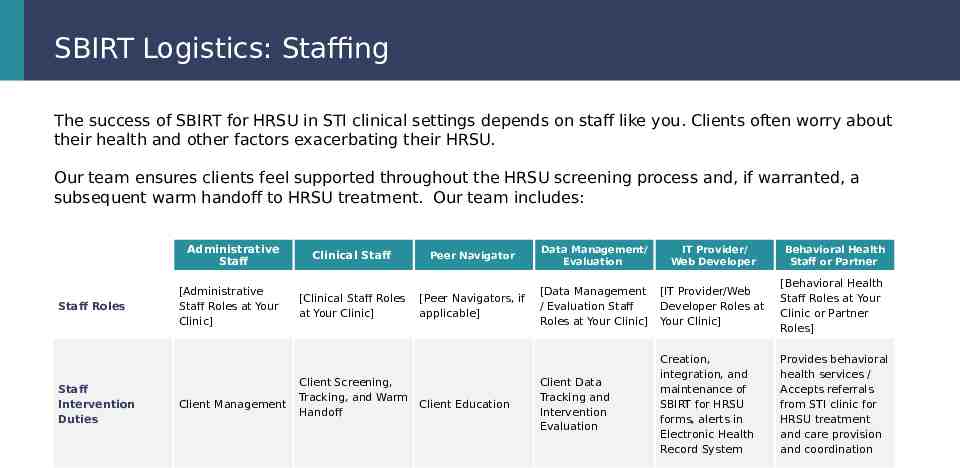
SBIRT Logistics: Staffing The success of SBIRT for HRSU in STI clinical settings depends on staff like you. Clients often worry about their health and other factors exacerbating their HRSU. Our team ensures clients feel supported throughout the HRSU screening process and, if warranted, a subsequent warm handoff to HRSU treatment. Our team includes: Administrative Staff Staff Roles Staff Intervention Duties [Administrative Staff Roles at Your Clinic] Client Management Clinical Staff [Clinical Staff Roles at Your Clinic] Client Screening, Tracking, and Warm Handoff Peer Navigator Data Management/ Evaluation IT Provider/ Web Developer [Peer Navigators, if applicable] [Data Management / Evaluation Staff Roles at Your Clinic] [IT Provider/Web Developer Roles at Your Clinic] [Behavioral Health Staff Roles at Your Clinic or Partner Roles] Client Data Tracking and Intervention Evaluation Creation, integration, and maintenance of SBIRT for HRSU forms, alerts in Electronic Health Record System Provides behavioral health services / Accepts referrals from STI clinic for HRSU treatment and care provision and coordination Client Education Behavioral Health Staff or Partner
SBIRT Logistics: Electronic Health Record System Our electronic health record system serves as the cornerstone of the SBIRT for HRSU intervention: Smart tags/phrases and pop-ups that serve as reminders about SBIRT and/or clients who may qualify for it. Integrated electronic forms that facilitate and record results of the SBIRT for HRSU screening process, including screening and SBIRT for HRSU results. Information about the results and other resources that clients may access through their customer medical record portal.
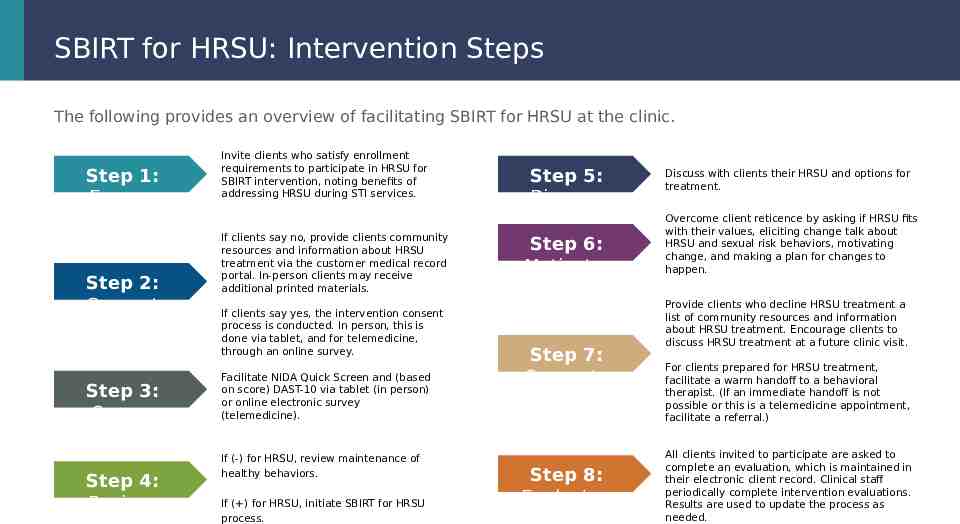
SBIRT for HRSU: Intervention Steps The following provides an overview of facilitating SBIRT for HRSU at the clinic. Step 1: Engage Step 2: Consent Step 3: Screen Step 4: Review Invite clients who satisfy enrollment requirements to participate in HRSU for SBIRT intervention, noting benefits of addressing HRSU during STI services. If clients say no, provide clients community resources and information about HRSU treatment via the customer medical record portal. In-person clients may receive additional printed materials. If clients say yes, the intervention consent process is conducted. In person, this is done via tablet, and for telemedicine, through an online survey. Facilitate NIDA Quick Screen and (based on score) DAST-10 via tablet (in person) or online electronic survey (telemedicine). If (-) for HRSU, review maintenance of healthy behaviors. If ( ) for HRSU, initiate SBIRT for HRSU process. Step 5: Discuss Step 6: Motivate Step 7: Connect Step 8: Evaluate Discuss with clients their HRSU and options for treatment. Overcome client reticence by asking if HRSU fits with their values, eliciting change talk about HRSU and sexual risk behaviors, motivating change, and making a plan for changes to happen. Provide clients who decline HRSU treatment a list of community resources and information about HRSU treatment. Encourage clients to discuss HRSU treatment at a future clinic visit. For clients prepared for HRSU treatment, facilitate a warm handoff to a behavioral therapist. (If an immediate handoff is not possible or this is a telemedicine appointment, facilitate a referral.) All clients invited to participate are asked to complete an evaluation, which is maintained in their electronic client record. Clinical staff periodically complete intervention evaluations. Results are used to update the process as needed.
Q&A Session
Follow Up and Contact Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod.
Citations 1 Copen CE, Brookmeyer KA, Haderxhanaj LT, Hogben M, Torrone EA. Sexual risk behaviors among persons diagnosed with primary and secondary syphilis who reported high-risk substance use: data from the National Notifiable Diseases Surveillance System, 2018. Sexually Transmitted Diseases. 2022 Feb 2;49(2):99. Liu S, Vivolo-Kantor A. A latent class analysis of drug and substance use patterns among patients treated in emergency departments for suspected drug overdose. Addictive Behaviors. 2020 Feb 1;101:106142. 2 Yu J, Appel P, Rogers M, Blank S, Davis C, Warren B, et al. Integrating intervention for substance use disorder in a healthcare setting: practice and outcomes in New York City STD clinics. Am J Drug Alcohol Abuse. 2016;42(1):32–8. 3 Babor TF, McRee BG, Kassebaum PA, Grimaldi PL, Ahmed K, Bray J. Screening, Brief Intervention, and Referral to Treatment (SBIRT): toward a public health approach to the management of substance abuse. Subst Abus. 2007;28(3):7–30. doi: 10.1300/J465v28n03 03. 4 NACCHO. Delivering Screening, Brief Intervention, and Referral to Treatment to Mitigate High-Risk Substance Use in STI Clinical Settings. 2024. Available at: https ://www.naccho.org/blog/articles/delivering-screening-brief-intervention-and-referral-to-treatment-to-mitigate-high-risk-substance-use-in-sti-clinical-se ttings 5 Feaster DJ, Parish CL, Gooden L, Matheson T, Castellon PC, Duan R, Pan Y, Haynes LF, Schackman BR, Malotte CK, Mandler RN. Substance use and STI acquisition: Secondary analysis from the AWARE study. Drug and Alcohol Dependence. 2016 Dec 1;169:171-9. 5 Werner RN, Gaskins M, Nast A, Dressler C. Incidence of sexually transmitted infections in men who have sex with men and who are at substantial risk of HIV infection–A metaanalysis of data from trials and observational studies of HIV pre-exposure prophylaxis. PloS One. 2018 Dec 3;13(12):e0208107. 6
Citations Burns A, Albrecht K. Localized syndemic assemblages: COVID-19, substance use disorder, and overdose risk in small-town America. RSF: The Russell Sage Foundation Journal of the Social Sciences. 2022 Dec 1;8(8):245-62. 11 Kidd SE, Grey JA, Torrone EA, Weinstock HS. Increased methamphetamine, injection drug, and heroin use among women and heterosexual men with primary and secondary syphilis—United States, 2013–2017. MMWR. 2019 Feb 2;68(6):144. 12 Learner ER, Grey JA, Bernstein K, Kirkcaldy RD, Torrone EA. Primary and secondary syphilis among men who have sex with men and women, 2010 to 2019. Sexually Transmitted Diseases. 2022 Nov 1;49(11):794-6. 13 Hill AV, Mendez DD, Haggerty CL, Miller E, De Genna NM. Syndemics of sexually transmitted infections in a sample of racially diverse pregnant young women. Maternal and Child Health Journal. 2022 Feb 1:1-0. 14 Butsang T, McLuhan A, Keown LA, Fung K, Matheson FI. Sex differences in pre-incarceration mental illness, substance use, injury and sexually transmitted infections and health service utilization: a longitudinal linkage study of people serving federal sentences in Ontario. Health & Justice. 2023 Apr 1;11(1):19. 15 Ellis MS, Kasper ZA, Takenaka B, Buttram ME, Shacham E. Associations of transactional sex and sexually transmitted infections among treatmentseeking individuals with opioid use disorder. American Journal of Preventive Medicine. 2023 Jan 1;64(1):17-25. 16 Walters SM, Kerr J, Cano M, Earnshaw V, Link B. Intersectional stigma as a fundamental cause of health disparities: A case study of how drug use stigma intersecting with racism and xenophobia creates health inequities for Black and Hispanic persons who use drugs over time. Stigma and Health. 2023 Mar 2. 17 Javanbakht M, Rosen A, Ragsdale A, Richter EI, Shoptaw S, Gorbach PM. Interruptions in mental health care, cannabis use, depression, and anxiety during the COVID-19 18
Citations 20 Singer M, Bulled N, Ostrach B, Mendenhall E. Syndemics and the biosocial conception of health. The Lancet. 2017 Mar 4;389(10072):941-50. 21 Sharma A. Syndemics: health in context. Lancet. 2017;389(10072):881. 22 Fishbein D. The pivotal role of prevention science in this syndemic. Prevention Science. 2021 Jan;22(1):94-9. Harvey L, Taylor JL, Assoumou SA, Kehoe J, Perera R, Schechter-Perkins EM, Bernstein E, Walley AY. Sexually transmitted and blood-borne infections among patients presenting to a low-barrier substance use disorder medication clinic. Journal of Addiction Medicine. 2021 Nov;15(6):461. 23 Kwan CK, Chan DP, Ho KM, Lee SS. Prevalence of sexually acquired hepatitis C virus (HCV) infection in sexually transmitted infection (STI) patients. Hong Kong Journal of Dermatology & Venereology. 2020 Jun 1;28. 24 25 Rietmeijer CA. Improving care for sexually transmitted infections. Journal of the International AIDS Society. 2019 Aug;22:e25349. Rogers BG, Murphy M, Zanowick-Marr A, Chambers L, Maynard M, Galipeau D, Toma E, Almonte A, Napoleon S, Chan PA. Characterizing HIV syndemics and the role of incarceration among men who have sex with men presenting for care at a sexually transmitted infections clinic. AIDS and Behavior. 2023 Jan 12:1-0. 26 Smith PC, Schmidt SM, Allensworth-Davies D, Saitz RA single-question screening test for drug use in pimary care. Arch Intern Med. 2010;170(13):1155-1160. doi:10.1001/archinternmed.2010.140 27 Bohn MJ, Babor T, Kranzler HR. Validity of the Drug Abuse Screening Test (DAST-10) in inpatient substance abusers. Problems of Drug Dependence. 1991;119:233-5. 28