Current & Future Hemophilia Therapy Options By: Ross Didonna, PharmD



20 Slides3.60 MB
Current & Future Hemophilia Therapy Options By: Ross Didonna, PharmD candidate September 29th, 2021
Outline - Types of bleeding disorders Data, statistics and disease severity Hemlibra Hemophilia A & B factor replacement Inhibitor development Roles of physical therapy Gene therapy Traveling restrictions The future of hemophilia treatment Patient case 2
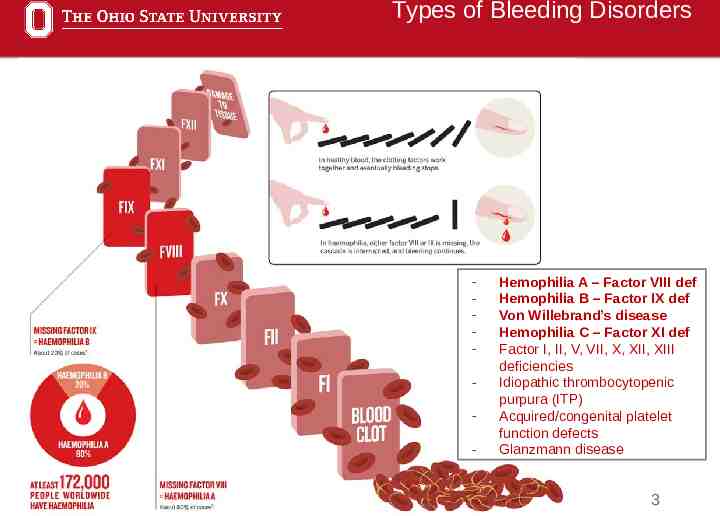
Types of Bleeding Disorders - Hemophilia A – Factor VIII def Hemophilia B – Factor IX def Von Willebrand’s disease Hemophilia C – Factor XI def Factor I, II, V, VII, X, XII, XIII deficiencies Idiopathic thrombocytopenic purpura (ITP) Acquired/congenital platelet function defects Glanzmann disease 3
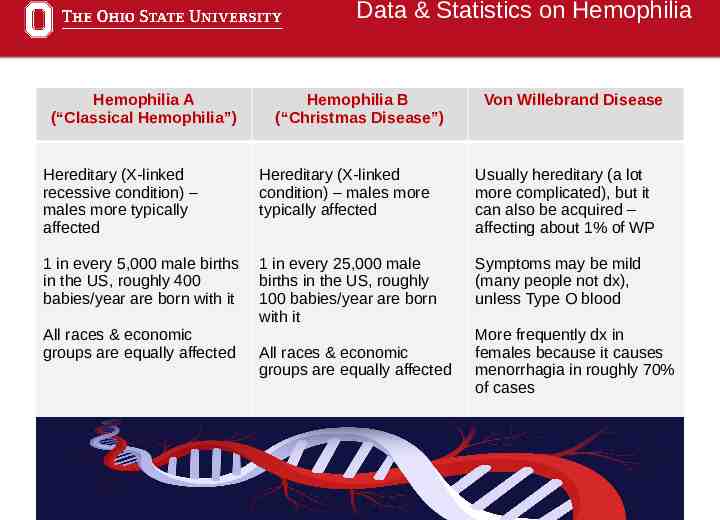
Data & Statistics on Hemophilia Hemophilia A (“Classical Hemophilia”) Hemophilia B (“Christmas Disease”) Von Willebrand Disease Hereditary (X-linked recessive condition) – males more typically affected Hereditary (X-linked condition) – males more typically affected Usually hereditary (a lot more complicated), but it can also be acquired – affecting about 1% of WP 1 in every 5,000 male births in the US, roughly 400 babies/year are born with it 1 in every 25,000 male births in the US, roughly 100 babies/year are born with it Symptoms may be mild (many people not dx), unless Type O blood All races & economic groups are equally affected All races & economic groups are equally affected More frequently dx in females because it causes menorrhagia in roughly 70% of cases 4
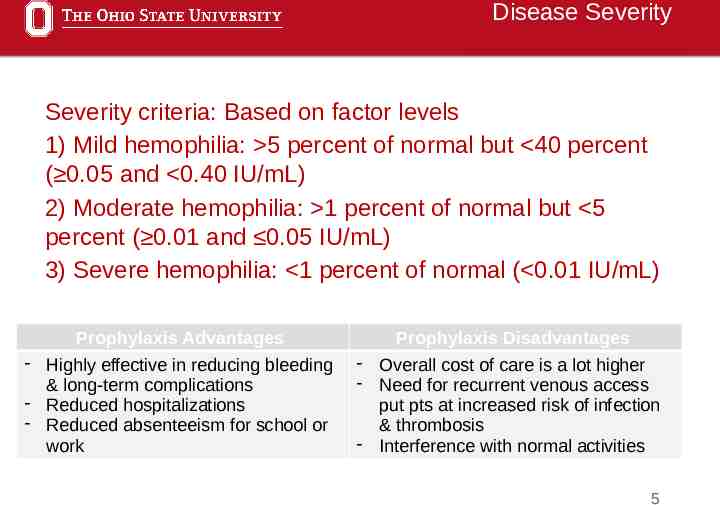
Disease Severity Severity criteria: Based on factor levels 1) Mild hemophilia: 5 percent of normal but 40 percent ( 0.05 and 0.40 IU/mL) 2) Moderate hemophilia: 1 percent of normal but 5 percent ( 0.01 and 0.05 IU/mL) 3) Severe hemophilia: 1 percent of normal ( 0.01 IU/mL) Prophylaxis Advantages Prophylaxis Disadvantages - Highly effective in reducing bleeding & long-term complications - Reduced hospitalizations - Reduced absenteeism for school or work - Overall cost of care is a lot higher - Need for recurrent venous access put pts at increased risk of infection & thrombosis - Interference with normal activities 5
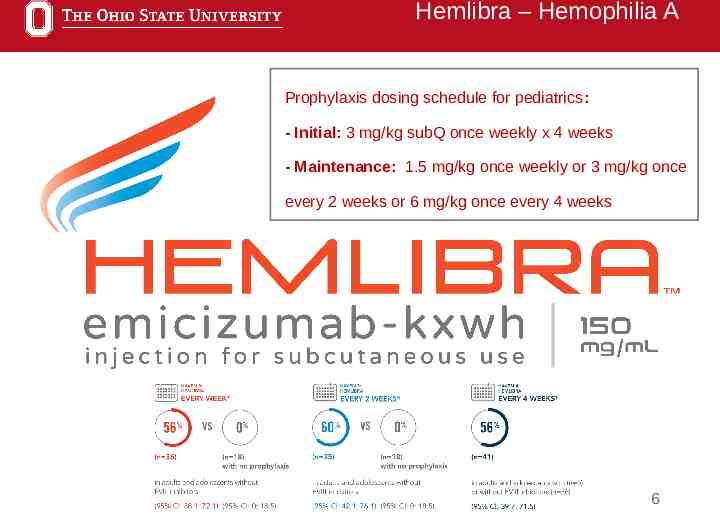
Hemlibra – Hemophilia A Prophylaxis dosing schedule for pediatrics: - Initial: 3 mg/kg subQ once weekly x 4 weeks - Maintenance: 1.5 mg/kg once weekly or 3 mg/kg once every 2 weeks or 6 mg/kg once every 4 weeks 6
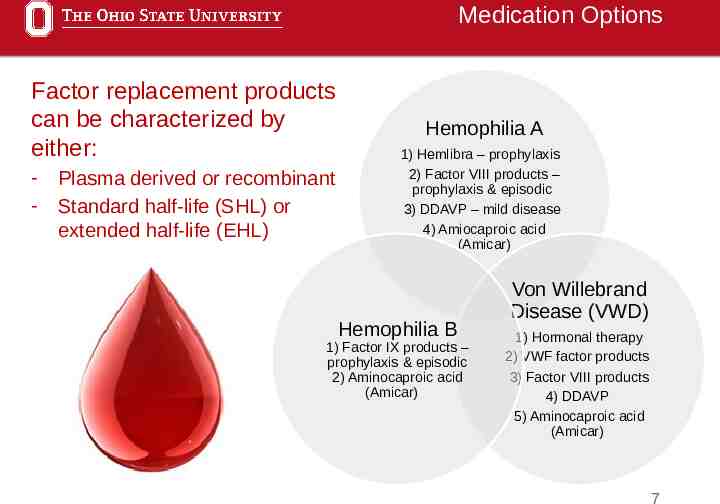
Medication Options Factor replacement products can be characterized by either: - Plasma derived or recombinant Standard half-life (SHL) or extended half-life (EHL) Hemophilia A 1) Hemlibra – prophylaxis 2) Factor VIII products – prophylaxis & episodic 3) DDAVP – mild disease 4) Amiocaproic acid (Amicar) Hemophilia B 1) Factor IX products – prophylaxis & episodic 2) Aminocaproic acid (Amicar) Von Willebrand Disease (VWD) 1) Hormonal therapy 2) VWF factor products 3) Factor VIII products 4) DDAVP 5) Aminocaproic acid (Amicar) 7
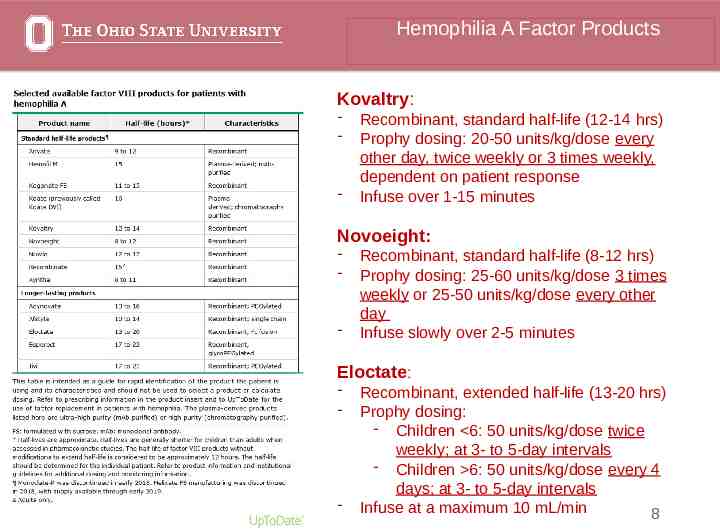
Hemophilia A Factor Products Kovaltry: - - Recombinant, standard half-life (12-14 hrs) Prophy dosing: 20-50 units/kg/dose every other day, twice weekly or 3 times weekly, dependent on patient response Infuse over 1-15 minutes Novoeight: - - Recombinant, standard half-life (8-12 hrs) Prophy dosing: 25-60 units/kg/dose 3 times weekly or 25-50 units/kg/dose every other day Infuse slowly over 2-5 minutes Eloctate: - - Recombinant, extended half-life (13-20 hrs) Prophy dosing: - Children 6: 50 units/kg/dose twice weekly; at 3- to 5-day intervals - Children 6: 50 units/kg/dose every 4 days; at 3- to 5-day intervals Infuse at a maximum 10 mL/min 8
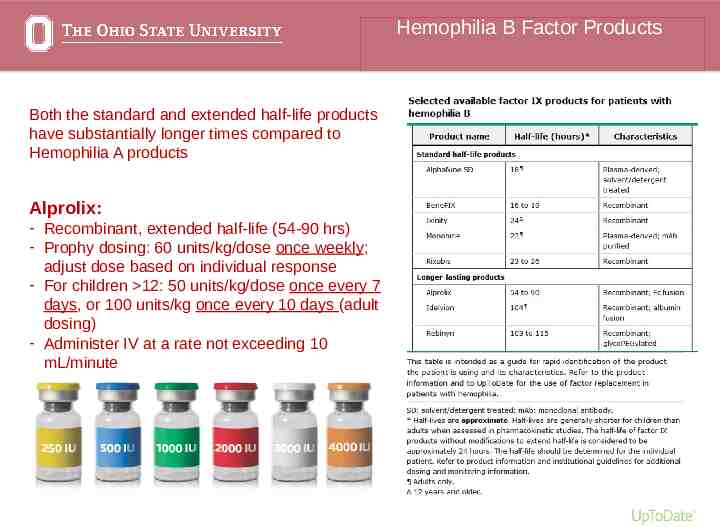
Hemophilia B Factor Products Both the standard and extended half-life products have substantially longer times compared to Hemophilia A products Alprolix: - Recombinant, extended half-life (54-90 hrs) - Prophy dosing: 60 units/kg/dose once weekly; adjust dose based on individual response - For children 12: 50 units/kg/dose once every 7 days, or 100 units/kg once every 10 days (adult dosing) - Administer IV at a rate not exceeding 10 mL/minute 9
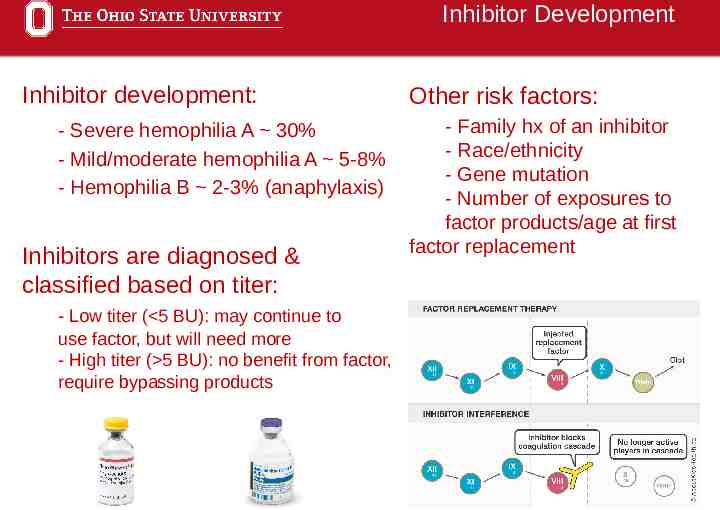
Inhibitor Development Inhibitor development: - Severe hemophilia A 30% - Mild/moderate hemophilia A 5-8% - Hemophilia B 2-3% (anaphylaxis) Inhibitors are diagnosed & classified based on titer: Other risk factors: - Family hx of an inhibitor - Race/ethnicity - Gene mutation - Number of exposures to factor products/age at first factor replacement - Low titer ( 5 BU): may continue to use factor, but will need more - High titer ( 5 BU): no benefit from factor, require bypassing products 10
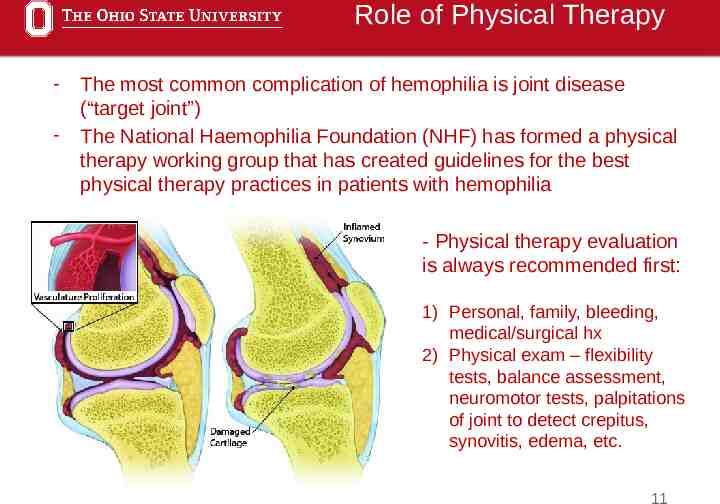
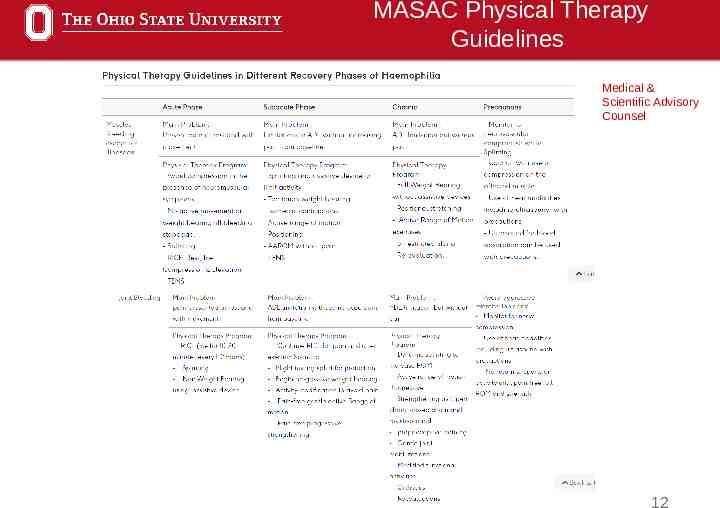
Role of Physical Therapy - The most common complication of hemophilia is joint disease (“target joint”) The National Haemophilia Foundation (NHF) has formed a physical therapy working group that has created guidelines for the best physical therapy practices in patients with hemophilia - Physical therapy evaluation is always recommended first: 1) Personal, family, bleeding, medical/surgical hx 2) Physical exam – flexibility tests, balance assessment, neuromotor tests, palpitations of joint to detect crepitus, synovitis, edema, etc. 11
MASAC Physical Therapy Guidelines Medical & Scientific Advisory Counsel 12
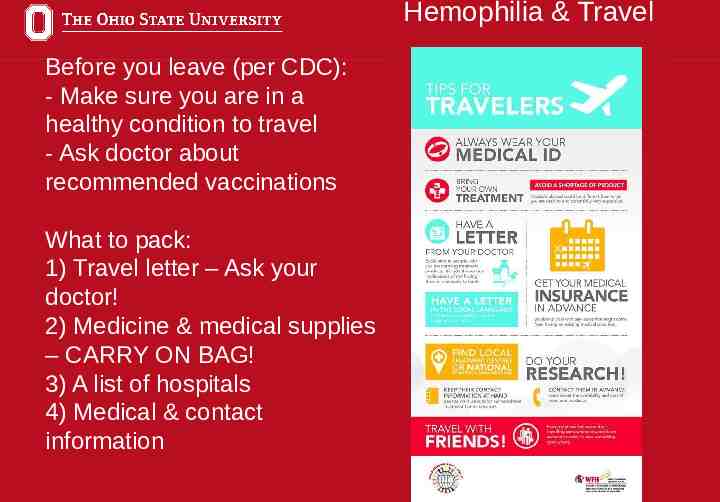
Hemophilia & Travel Before you leave (per CDC): - Make sure you are in a healthy condition to travel - Ask doctor about recommended vaccinations What to pack: 1) Travel letter – Ask your doctor! 2) Medicine & medical supplies – CARRY ON BAG! 3) A list of hospitals 4) Medical & contact information 13
The Future of Gene Therapy Different types of gene therapy: 1) Gene transfer 2) Cell therapy 3) Gene editing (CRISPR) 14
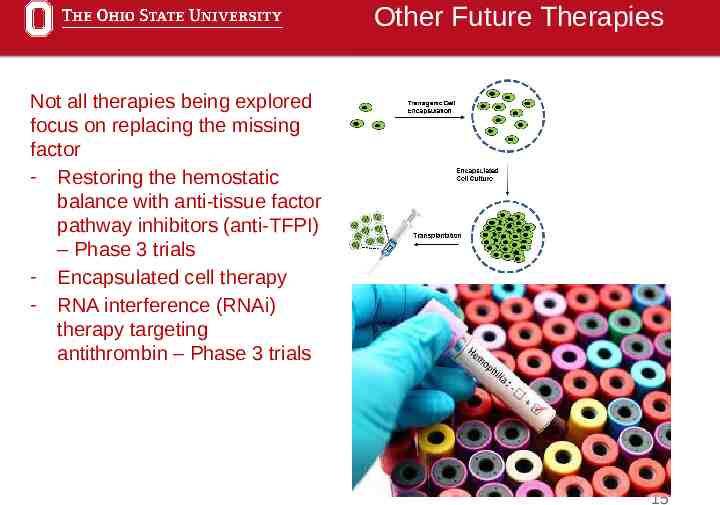
Other Future Therapies Not all therapies being explored focus on replacing the missing factor - Restoring the hemostatic balance with anti-tissue factor pathway inhibitors (anti-TFPI) – Phase 3 trials - Encapsulated cell therapy - RNA interference (RNAi) therapy targeting antithrombin – Phase 3 trials 15
Patient Case HM is a 15 yo, 168 lbs (76.5 kg) male with PMH of severe hemophilia A with inhibitor development. Pt has had some complications such as a subdural hematoma and intracranial hemorrhage in the past. Family hx is as followed: - Mother (alive): Hemophilia A carrier - Father (deceased): Heart disease & stroke - HM has 3 brothers: 2 with Hemophilia A (1 deceased), 1 w/o hemophilia - HM has 4 sisters: 3 w/o hemophilia (1 decreased), 1 a symptomatic carrier HM’s treatment timeline: - 2006-2010: Alphanate, Novo7 prn, Cipro locks (BSI’s stopped in 2009) - 2010-2016: Alphanate, Eloctate, Novo7 prn - 2016-2017: Advate, Novo7 prn - Current: - Hemlibra 115 mg subQ Qweekly - Eloctate 7,670 units IV daily prn before physical therapy - Novo7 7,000 units IV daily prn before physical therapy 16
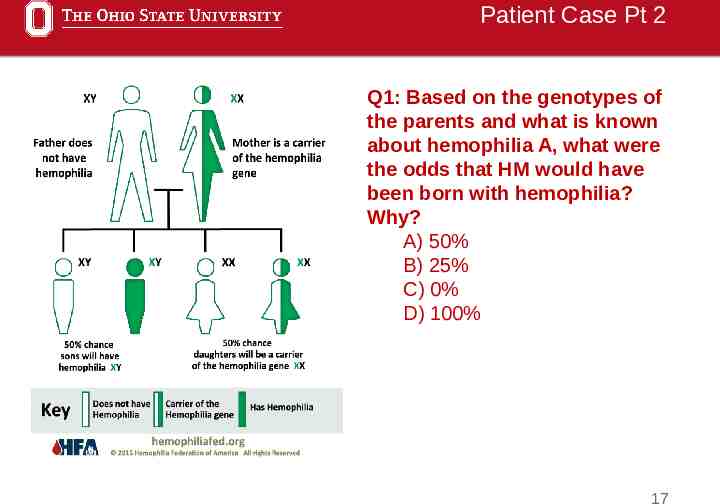
Patient Case Pt 2 Q1: Based on the genotypes of the parents and what is known about hemophilia A, what were the odds that HM would have been born with hemophilia? Why? A) 50% B) 25% C) 0% D) 100% 17
Patient Case Pt 3 Q2: HM’s current medications include Hemlibra and Eloctate. His most recent inhibitor titer came back as 10 BU. What classification does HM fall into, and which medication would no longer be appropriate? A) Low titer, Eloctate B) High titer, Eloctate C) Low titer, Hemlibra D) High titer, Hemlibra - HM has really benefited from Hemlibra and has been on his current therapy for a couple of years now - His younger brother is also on Hemlibra and is tolerating it well 18
Questions? 19
References - BioMarin Pharmaceuticals Inc. What is Gene Therapy? Hemdifferently. https://www.hemdifferently.com/what-is-gene-therapy/. Accessed September 22, 2021. - Current Treatments. National Hemophilia Foundation. https://www.hemophilia.org/bleeding-disorders-a-z/treatment/currenttreatments. Accessed September 22, 2021. - Efficacy for Adults and Adolescents Without FVIII Inhibitors. Hemlibra. https://www.hemlibra-hcp.com/trials-and-results/patients-without-fviiiinhibitors.html. Accessed September 23, 2021. - Hemophilia Foundation of America (HFA). Dateline Federation. Volume 22, Issue 1. https://www.hemophiliafed.org/dateline/HFA Dateline 2021 Q1 Spring Spe cial/ - Haemophilia. Physiopedia. https://www.physio-pedia.com/Haemophilia. Accessed September 22, 2021. 20