Colorectal Cancer Update for Healthcare Providers May 2013































44 Slides1.86 MB
Colorectal Cancer Update for Healthcare Providers May 2013 Maryland Department of Health and Mental Hygiene Prevention and Health Promotion Administration Cigarette Restitution Fund Program Center for Cancer Prevention and Control
CRC Incidence, Mortality, and Survival in the U.S. Prevention and Health Promotion Administration May 2013 2
Colorectal Cancer Third most commonly diagnosed cancer in Maryland among both men and women Second leading cause of cancer-related mortality Incidence and mortality have been decreasing in recent years Prevention and Health Promotion Administration May 2013 3
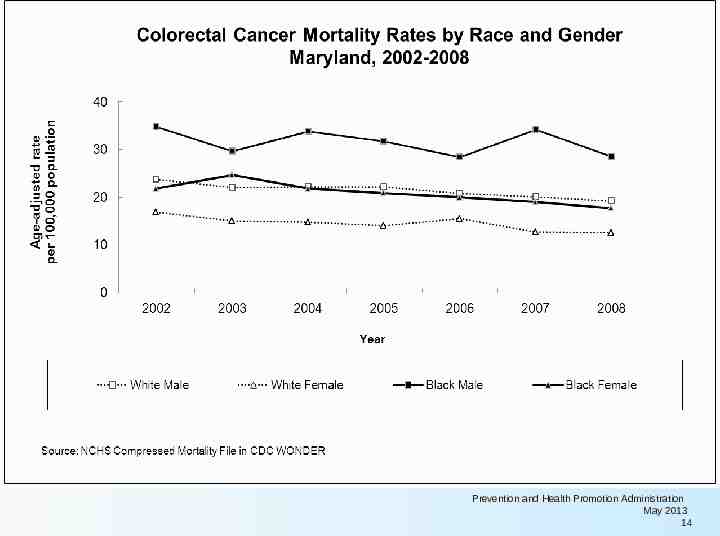
Colorectal Cancer Incidence and Mortality Rates by Year of Diagnosis or Death, Maryland, 2002-2008 Maryland Cancer Registry (incidence rates) NCHS Compressed Mortality File in CDC WONDER (mortality rates) Prevention and Health Promotion Administration May 2013 4
Colorectal Cancer 5-year CRC survival has improved over the past 30 years in the U.S. Source: SEER 9 areas. SEER Program, National Cancer Institute. Prevention and Health Promotion Administration May 2013 5
CRC Screening Prevention and Health Promotion Administration May 2013 6
Colorectal Cancer Screening Status of People Age 50 Years and Older Maryland Cancer Surveys and BRFSS, 2002-2010 18 20 Never tested 8 Tested but not upto-date* 22 23 26 9 11 10 10 5 Up-to-date with FOBT and/or sigmoidoscopy 7 11 17 23 Up-to-date with colonoscopy 41 0 10 20 30 40 50 59 50 60 2008 2010 66 67 70 Percent 2002 Maryland Cancer Survey, 2002-2008 BRFSS, 2010 2004 2006 Prevention and Health Promotion Administration May 2013 7
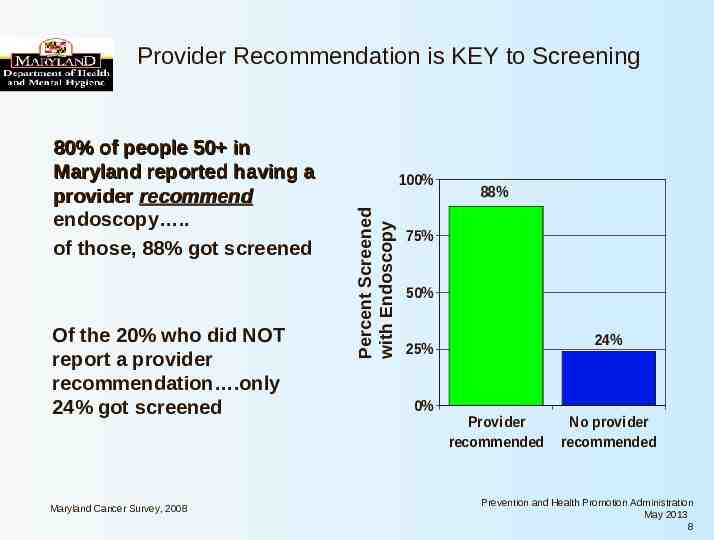
Provider Recommendation is KEY to Screening Of the 20% who did NOT report a provider recommendation .only 24% got screened Maryland Cancer Survey, 2008 100% Percent Screened with Endoscopy 80% of people 50 in Maryland reported having a provider recommend endoscopy . of those, 88% got screened 88% 75% 50% 24% 25% 0% Provider recommended No provider recommended Prevention and Health Promotion Administration May 2013 8
Colorectal Cancer Screening with colonoscopy or sigmoidoscopy? (50 years) Never screened with colonoscopy or sigmoidoscopy 25% Maryland Cancer Survey, 2008 Ever screened with colonoscopy or Sigmoidoscopy 75% Prevention and Health Promotion Administration May 2013 9
Colorectal Cancer Screening with colonoscopy or sigmoidoscopy? (50 years) Never screened with colonoscopy or sigmoidoscopy 25% 85% have been to doctor for “routine checkup” in past 2 years Maryland Cancer Survey, 2008 Ever screened with colonoscopy or Sigmoidoscopy 75% Only 15% have NOT had checkup Prevention and Health Promotion Administration May 2013 10
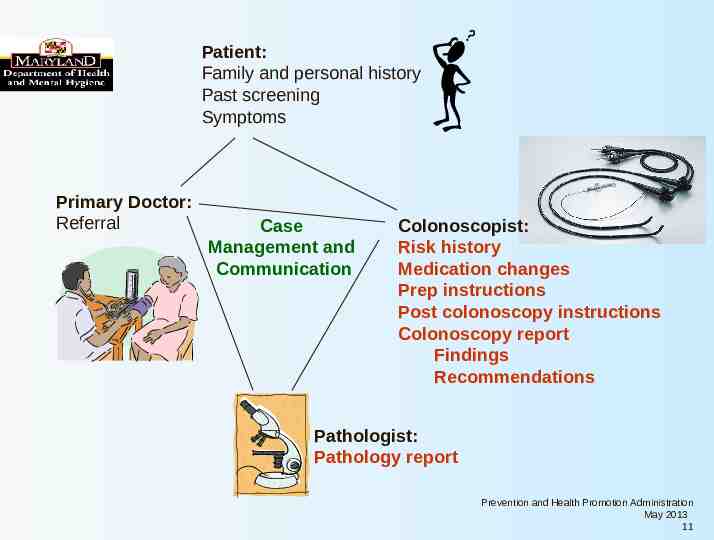
Patient: Family and personal history Past screening Symptoms Primary Doctor: Referral Case Management and Communication Colonoscopist: Risk history Medication changes Prep instructions Post colonoscopy instructions Colonoscopy report Findings Recommendations Pathologist: Pathology report Prevention and Health Promotion Administration May 2013 11
Who needs screening? Prevention and Health Promotion Administration May 2013 12
Colorectal Cancer Age-Specific Incidence Rates by Gender, Maryland and U.S., 2004-2008 450 Age-specific rate per 100,000 population 400 350 300 250 200 150 100 50 0 Age Group MD Male MD Female U.S. Male U.S. Female Source: Maryland Cancer Registry Prevention and Health Promotion Administration May 2013 13
Prevention and Health Promotion Administration May 2013 14
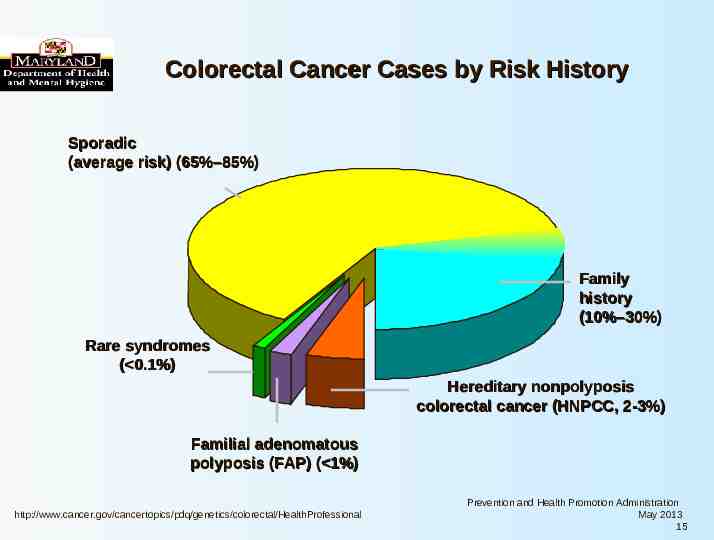
Colorectal Cancer Cases by Risk History Sporadic (average risk) (65%–85%) Family history (10%–30%) Rare syndromes ( 0.1%) Hereditary nonpolyposis colorectal cancer (HNPCC, 2-3%) Familial adenomatous polyposis (FAP) ( 1%) http://www.cancer.gov/cancertopics/pdq/genetics/colorectal/HealthProfessional Prevention and Health Promotion Administration May 2013 15
Risk of CRC Group Approx. lifetime risk of CRC General Population 5-6% One first degree relative (FDR) with CRC 2--3-fold increase over general population Two FDRs with CRC 3--4-fold increase FDR with CRC diagnosed 50 3--4-fold increase One second or third degree relative About 1.5-fold increase Two second degree relatives About 2--3-fold increase Inflammatory Bowel Disease (ulcerative colitis and Crohn’s colitis) 7-10% have CRC after having ulcerative colitis for 20 years; then 1%/year Familial adenomatous polyposis (FAP) Hereditary non-polyposis colorectal cancer (HNPCC) 100% 80 % Burt RW. Gastroenterology 2000;119:837-53 Winawer S, et al. Gastroenterology 2003;124:544-560 Prevention and Health Promotion Administration May 2013 16
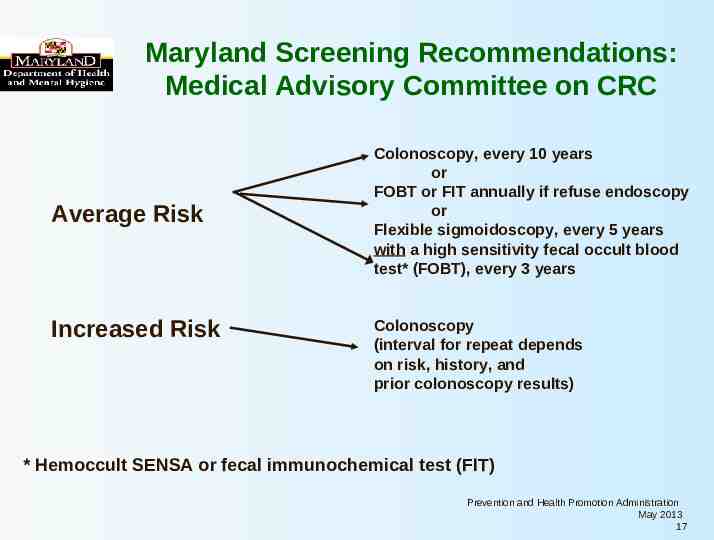
Maryland Screening Recommendations: Medical Advisory Committee on CRC Average Risk Increased Risk Colonoscopy, every 10 years or FOBT or FIT annually if refuse endoscopy or Flexible sigmoidoscopy, every 5 years with a high sensitivity fecal occult blood test* (FOBT), every 3 years Colonoscopy (interval for repeat depends on risk, history, and prior colonoscopy results) * Hemoccult SENSA or fecal immunochemical test (FIT) Prevention and Health Promotion Administration May 2013 17
Age to Begin Screening by Risk Category Risk Category Average risk Age to Begin Screening Age 50 years Increased risk Family History Colorectal cancer or adenomatous polyp(s)* in an FDR age 60, or in 2 or more FDRs at any age * Especially if advanced adenomas: 1 cm; villous histology; or high grade dysplasia Genetic syndrome: Familial adenomatous polyposis (FAP) Hereditary non-polyposis colorectal cancer (HNPCC) Inflammatory bowel disease Age 40 years, or 10 years before the youngest case in the immediate family, whichever is earlier Age 10 to 12 years Age 20 to 25 years, or 10 years before the youngest case in the immediate family Cancer risk begins to be significant 8 years after the onset of pancolitis (involvement of entire large intestine), or 12-15 years after the onset of leftsided colitis Rex DK, et al. Am J Gastroenterol 2009:104;739-750 American Cancer Society, 2012 http://www.cancer.org/Cancer/ColonandRectumCancer/MoreInformation/ ColonandRectumCancerEarlyDetection/colorectal-cancer-early-detection-acs-recommendations Prevention and Health Promotion Administration May 2013 18
Guidelines Screening and Surveillance for the Early Detection of Colorectal Cancer and Adenomatous Polyps, 2008: A Joint Guideline from the American Cancer Society, the U.S. Multi-Society Task Force on CRC, and the American College of Radiology CA Cancer J Clin 58: 130-160 (May 2008) Prevention and Health Promotion Administration May 2013 19
Tests that Find Both Polyps and Cancer Flexible sigmoidoscopy every 5 years Colonoscopy every 10 years Double contrast barium enema every 5 years CT colonography (virtual colonoscopy) every 5 years Guidelines, American Cancer Society, June 2012 http://www.cancer.org/Cancer/ColonandRectumCancer/MoreInformation/ ColonandRectumCancerEarlyDetection/colorectal-cancer-early-detection-screeningtests-used Prevention and Health Promotion Administration May 2013 20
Tests that Primarily Find Cancer High sensitivity FOBT every year Hemoccult SENSA or fecal immunochemical test (FIT) Stool DNA test (unclear how often this is needed, not currently available commercially is U.S.) Guidelines, American Cancer Society, 2012 http://www.cancer.org/cancer/colonandrectumcancer/detailedguide/colorectal-cancerdetection-recommendations United States Preventive Services Task Force http://www.uspreventiveservicestaskforce.org/uspstf08/colocancer/coloartzaub.htm#result s Prevention and Health Promotion Administration May 2013 21
CRC Screening Guidelines American Cancer Society, June 2012 Beginning at age 50, men and women at average risk for CRC should use one of the screening tests. The tests that are designed to find both early cancer and polyps are preferred if these tests are available to the patient and the patient is willing to have one of these more invasive tests. Talk to your doctor about which test is best for you. Prevention and Health Promotion Administration May 2013 22
CRC Screening under the Cigarette Restitution Fund Program (CRFP) in Maryland Prevention and Health Promotion Administration May 2013 23
Prevention and Health Promotion Administration May 2013 24
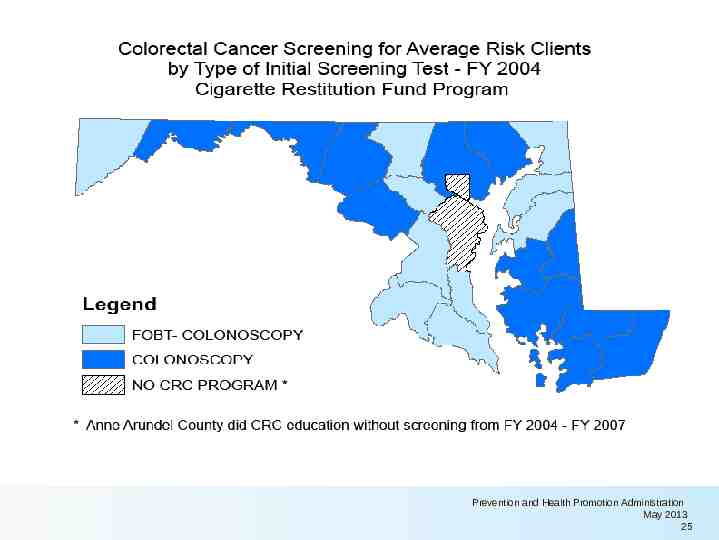
Prevention and Health Promotion Administration May 2013 25
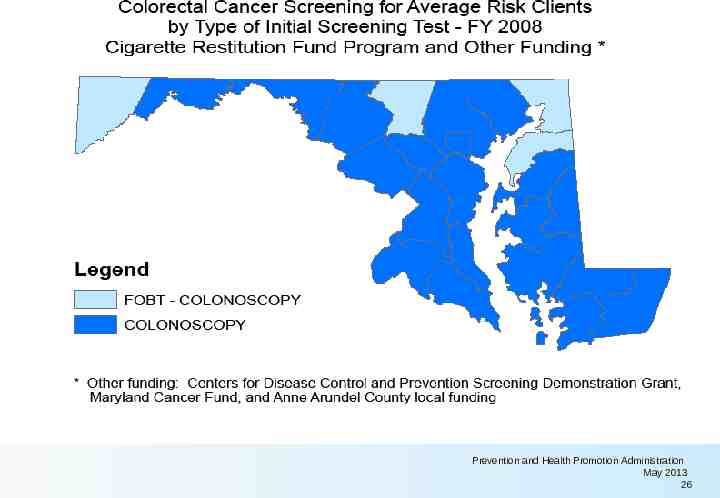
Prevention and Health Promotion Administration May 2013 26
Prevention and Health Promotion Administration May 2013 27
Summary of Cigarette Restitution Fund Colorectal Cancer Screening in Maryland As of December 31, 2012: 23,203 People have had one or more screening procedures 8,356 181 21,355 FOBTs (all income levels) Sigmoidoscopies Colonoscopies DHMH, CCPC, Client Database, C-CoPD, as of 2/25/2013 Prevention and Health Promotion Administration May 2013 28
Summary of Cigarette Restitution Fund Colorectal Cancer Screening County, Maryland 2000-20XX: r u o P XX Individuals screened for CRC y ient o r C o f Cl Cs by one or more method r e be th and m u from PD ine 1 n in ion -Co rra 079 XX FOBTs* a t o t Ob isdic se, C all L -767 XX Colonoscopies* jur taba , or c 410 Da orts ood X Cancers* rep derw Un X High grade dysplasia* XX Adenoma(s)* DHMH, CCPC, Client Database, C-CoPD, as of xx/xx/xxxx DHMH, CCPC, Client Database, C-CoP, as of xx/xx/xxxx Prevention and Health Promotion Administration May 2013 29
Gender of 23,173 Screened* for CRC Maryland, 2000-December 2012 Men 7,587 (33%) Women 15,586 (67%) *Of clients with known gender screened with one or more of the following: FOBT, flexible sigmoidoscopy, colonoscopy, imaging DHMH, CCPC, Client Database, C-CoPD, as of 2/26/2013 Prevention and Health Promotion Administration May 2013 30
Minority Status of 23,203 New People Screened* for CRC, Maryland, 2000-December 2012 Non-minority or Unknown 11,110 (48%) Minority 12,093 (52%) *Of clients screened with one or more of the following: FOBT, flexible sigmoidoscopy, colonoscopy, imaging DHMH, CCPC, Client Database, C-CoPD, as of 2/26/2013 Prevention and Health Promotion Administration May 2013 31
Results* of 21,356 Colonoscopies Maryland Cigarette Restitution Fund Program Maryland, 2000-December 2012 Inadequate col but no f indings, 306, 1% Negativ e, 3294, 15% Cancer/Suspect Cancer, 243, 1% Adenoma HighGrade, 88, 0% Adenomas, Other, 5,074, 24% Other f indings, 7,771, 36% Other poly ps, 4,580, 22% * Most “advanced” finding on colonoscopy DHMH, CCPC, Client Database, C-CoP, as of 2/27/2013 Prevention and Health Promotion Administration May 2013 32
“Recall Interval” Recommended screening after initial screening-rescreening or surveillance colonoscopy Prevention and Health Promotion Administration May 2013 33
After first colonoscopy, then what? what Interval between colonoscopies will depend on: – findings on last colonoscopy, – risk history, and – symptoms Prevention and Health Promotion Administration May 2013 34
For the recommended recall intervals, please see: DHMH Colorectal Cancer Minimal Elements http://phpa.dhmh.maryland.gov/cancer/Shared%20Documents/ccpc1324--att CRCMinimalElements2013[1].pdf (or http://phpa.dhmh.maryland.gov/cancer/ under Resources) Prevention and Health Promotion Administration May 2013 35
Guidelines for Recall Intervals Following Colonoscopy Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology, 2012;143:844–857 Rex DK, Ahnen DJ, Baron JA, Batts KP, Burke CA, et al. Serrated lesions of the colorectum: Review and recommendations from an expert panel. Am J Gastroenterol. 2012:109;1315-29. Prevention and Health Promotion Administration May 2013 36
Keys to the right recall 1. 2. 3. 4. Colonoscopy Report Pathology Report Recommendation based on guidelines Communication Prevention and Health Promotion Administration May 2013 37
Standards for Colonoscopy Reports— CO-RADS* Colonoscopy report should include: Date and Time - Procedure Patient description Risk factors ASA class Indications Consent signed Sedation Colonoscope Bowel prep adequacy Whether cecum reached Colonoscopy withdrawal time Findings Specimen(s) to path lab Impression Complications Pathology Recommendations Follow-up plan/Recall Other *Standardized colonoscopy reporting and data system: report of the Quality Assurance Task Group of the National Colorectal Cancer Roundtable, Lieberman et al., Gastrointestinal Endoscopy 2007; 65: 757-766 Prevention and Health Promotion Administration [Date] 38
Adequacy of First Colonoscopy Among 16,813* First Cycle Colonoscopies Maryland, 2000-December 2012 Not Adequate 1,555 (9%) (Inadequate prep OR didn't reach cecum) Adequate 15,258 (91%) *16,813 of the 17,915 first colonoscopies had information on “adequacy” of the col in CRFP. DHMH, CCPC, Client Database, Data Download, 2/27/2013 Prevention and Health Promotion Administration May 2013 39
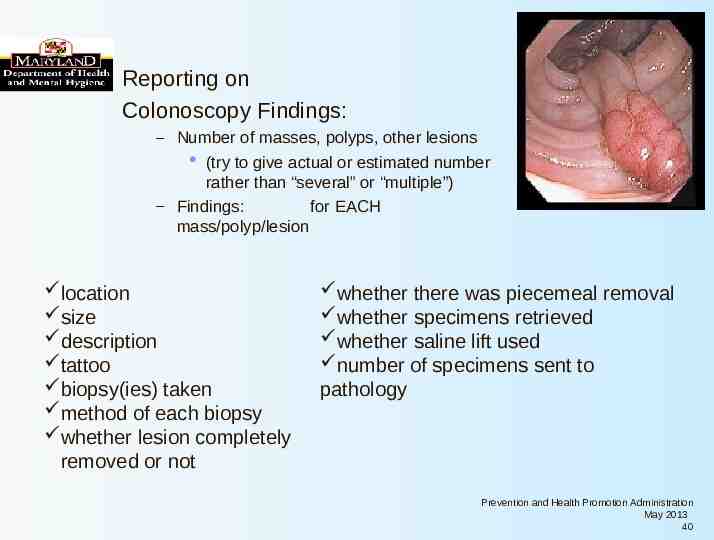
Reporting on Colonoscopy Findings: – Number of masses, polyps, other lesions (try to give actual or estimated number rather than “several” or “multiple”) – Findings: for EACH mass/polyp/lesion location size description tattoo biopsy(ies) taken method of each biopsy whether lesion completely removed or not whether there was piecemeal removal whether specimens retrieved whether saline lift used number of specimens sent to pathology Prevention and Health Promotion Administration May 2013 40
How will your patients be reminded about their next colonoscopy? Prevention and Health Promotion Administration May 2013 41
Patient: Family and personal history Past screening Symptoms Primary Doctor: Referral Colonoscopist: Case Risk history Management and Medication changes Communication Prep instructions Post colonoscopy instructions Colonoscopy report Findings Recommendations Pathologist: Pathology report Prevention and Health Promotion Administration May 2013 42
Acknowledgements Funding from the Maryland Cigarette Restitution Fund (CRF) Staff and partners of Local Public Health Department Programs in MD and their contracted providers DHMH Center for Cancer Prevention and Control (CCPC) Database and Quality assurance Surveillance and Evaluation Unit including - University of Maryland at Baltimore - Ciber, Inc. CCPC CRF Programs Unit Maryland Cancer Registry Minority Outreach Technical Assistance Partners Prevention and Health Promotion Administration May 2013 43
PREVENTION AND HEALTH PROMOTION ADMINISTRATION http://phpa.dhmh.maryland.gov