Clinical Documentation 2006 Annual Texas Institute on Substance

53 Slides271.50 KB
Clinical Documentation 2006 Annual Texas Institute on Substance Abuse and Mental Health Rhonda G. Patrick, LCSW Press ENTER for next slide. 1
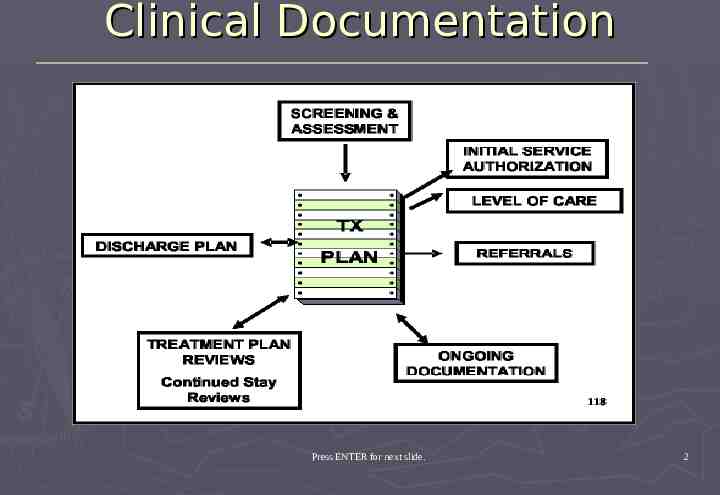
Clinical Documentation Press ENTER for next slide. 2
ASSESSMENT Press ENTER for next slide. 3
What is the assessment? An ASSESSMENT is the gathering of relevant information about the client, their environment, their problem(s), and what they hope to accomplish through the therapeutic intervention. Press ENTER for next slide. 4
Goals of the Assessment The assessment should answer the following questions: Is treatment of any kind required? What are the relative merits of the intervention? What types of treatment approaches might be appropriate? What is the depth of therapy needed? Who should the therapy involve? Have cultural issues been considered? Press ENTER for next slide. 5
Goals of the Assessment The Assessment should answer these basic Questions: Why is the client seeking treatment? How have these problems affected the client’s life? What is maintaining these problems? What does the client hope to gain from treatment? Press ENTER for next slide. 6
Who can conduct an Assessment? Licensed Counselor (LCDC, LPC, LMSW, Ph.D) Registered Counselor Intern Both are: Knowledgeable to assess the specific needs of the client being served Are trained in the use of applicable and appropriate tools Are culturally sensitive to the client’s needs Press ENTER for next slide. 7
Parts of the Assessment Presenting Problem or Chief Complaint Alcohol and Other Drug Use History (use) Family and Social/Leisure History (activities) Educational/Employment History (training) Legal History Mental Health History (mental/emotional functioning) Medical History (HIV, STD, TB, HEP) Client Strengths and Limitations Recommendations Press ENTER for next slide. 8
Presenting Problem Asks the client: What brings you here today? Why do you think you need treatment? Press ENTER for next slide. 9
Alcohol and Drug Use Substances used in the past Substances used recently Frequency/amount/duration Route of administration Year or Age of first use Behavior related to obtaining substances Use or recovering from alcohol or other drugs Previous overdose, withdrawal, or adverse drug or alcohol reactions Attempts to decrease/stop use History of previous substance abuse treatment received Press ENTER for next slide. 10
Family, Social & Leisure The family history should include: The occupation and education of patents The number of siblings and their birth order The quality of clients relationship to parents and or siblings Significant extended family members Parental approach to child rearing Familial expectations for the client Press ENTER for next slide. 11
Educational Educational history can give: Rough estimate of the client’s level of intelligence Aspirations, goals, ability to gain from learning experiences Willingness to make a commitment Amount of perseverance Ability to delay gratification Press ENTER for next slide. 12
Employment Employment history can: be useful in developing an effective treatment plan give insight into the client’s ability to get along with others and take direction show client’s ability for assuming the role of a client show compliance with treatment recommendations Press ENTER for next slide. 13
Legal History Currently legal problems probation parole awaiting trial/sentencing recently released from jail/prison Complications with legal situation positive UA Are legal problems directly related to substance use? Press ENTER for next slide. 14
Mental Health History Can shed light on whether the current problem is part of a single or recurrent episode. A progression of behavioral health problems over a period of time. What treatment approaches have or have not worked. Client’s willingness to engage in the treatment process. Get an idea of current emotional functioning. Press ENTER for next slide. 15
Medical History At a minimum document: any significant illnesses hospitalizations past and current physical illnesses or conditions breast or prostate cancer diabetes hypertension injuries or disorders affecting the central nervous system any functional limitations HIV, STD, TB or Hepatitis exposure or contact cursory family history of significant medical problems Press ENTER for next slide. 16
Recommendations The assessment must include: The clinical recommendations counseling education treatment Recommendation for treatment must indicate the level of care Detox Residential Outpatient What are the recommended: services length of stay intensity of services Diagnostic Justification Summary Press ENTER for next slide. 17
DSM-IV Multi-axial Diagnostic System Axis I Axis II Axis III Axis IV Axis V (Clinical Disorders, other conditions that may be a focus of attention) Examples: Substance abuse, substance dependence, anxiety disorders, mood disorders, schizophrenia (Personality disorders, mental retardation) Examples: Borderline personality disorder, antisocial personality disorder, avoidant personality disorder, mental retardation (General medical conditions) Examples: Cancer, Hypertension, Diabetes, Migraines, Chronic Pain, Injuries (Psychosocial and environmental problems) Examples: Problems with primary support group, occupational problems, problems relating to social environment Score (Global assessment of functioning) Example: GAF Press ENTER for next slide. 18
Other Issues Problem Complexity Readiness to Change Resistance to Change Social Supports Coping Styles Motivation Press ENTER for next slide. 19
Treatment Planning Press ENTER for next slide. 20
The purpose of Treatment Planning To clarify the treatment focus The set realistic expectations To establish a standard for measuring treatment progress The facilitate communication among professions (both Clinical and Support) To support treatment authorizations To document quality assurance efforts Press ENTER for next slide. 21
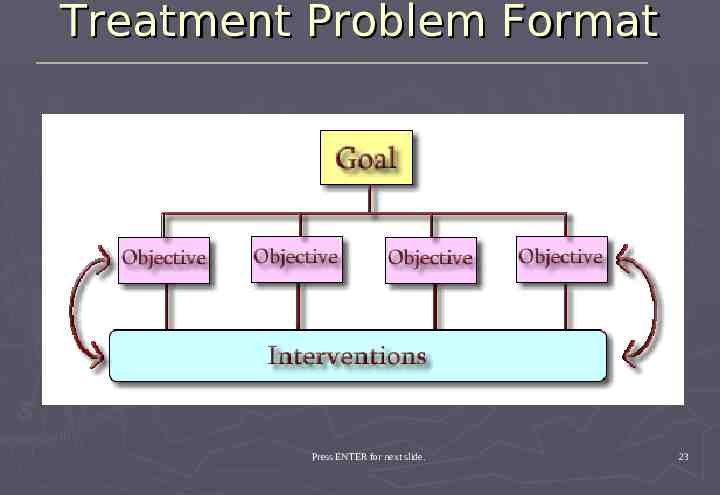
Treatment Plan Content Problem List Presenting Problem Goals Objectives Treatment Interventions Criteria for Discharge Press ENTER for next slide. 22
Treatment Problem Format Press ENTER for next slide. 23
Problem List Problems that are judged by any of the potential referring parties to: have a significant impact on the client’s ability to function appropriately and adequately in any sphere of life (e.g., family, social, work, school) be amenable to behavioral health care intervention should be listed here The identified problems should be stated in clear and unambiguous language in the treatment plan Example: “problems in school” could mean a lot of things for a given client, instead “academic underachievement,” “disruptive behavior during class,” for “aggressive behavior outside the classroom” provides a better description of the problem that would be the focus of the treatment. Press ENTER for next slide. 24
Presenting Problem Should contain a statement about the problem for which the client is seeking treatment. Clarification of how the problem is evidenced for this specific client. Identification of the symptoms that fit DSM-IV criteria Should always be documented in the client’s own words. The client’s own problem description frequently can: convey more information about themselves the intensity of the problem and how these problems affect their life then Press ENTER for next slide. 25
Treatment Goals The counselor and client will identify of treatment goals. Goals can be client-identified or third-party goals. It is important to have clients identify what the anticipated or hoped-for results of achieving their goals will be. Press ENTER for next slide. 26
Client-Identified Goals Ask the client directly what their goals are using these three questions: 1. 2. 3. What do you see as our biggest problem? What do you want to be different about your life at the end of your treatment? Does this goal involve changing things about yourself? Press ENTER for next slide. 27
Client-Identified Goals, Cont. Does this goal involve changing things about yourself? This question forces the client to think through their problems and realize the extent to which these problems have control over their thoughts, feelings, and behavior(s). It can provide a means for clients to gain insight into their problems – a therapeutic goal in and of itself. Press ENTER for next slide. 28
Client-Identified Goals, Cont. Ask clients the following questions relating to establishing objective outcome criteria for goal achievement: How will you know when things are different? 2. What kinds of things will you be doing differently? 3. What negative things will no longer be present? 4. What positive things will you be doing? These questions offer clients an opportunity to gain insight into their problems. Clinician feedback can help clients see how realistic their expectations are for treatment and determine Press ENTER for next slide. whether those expectations should be modified. 1. 29
Third Party Goals Treatment goals set by non-client stakeholders in the treatment process must always be considered, examples: spouses judicial system employer family members Third party expectations of outcomes should be sought and/or modified based on the clinician’s evaluation of how realistic they are. Press ENTER for next slide. 30
Treatment Plan Objectives The following questions can be used to determine if they are realistic: 1. 2. Does the client have the motivation to do the work that is required? Does the client have a support system to assist them? The reality of the situation must be taken into consideration when determining whether a specific goal, objective, or time frame should become part of the treatment plan. Press ENTER for next slide. 31
Treatment Plan Objectives Goals and objectives should be: stated in measurable terms goals and objectives should be quantifiable, specific and easily understood by the client and all stakeholders Measurability allows for: tracking client progress through the treatment process providing information regarding the effectiveness of the treatment plan allows the client to see what they have accomplished through the treatment process Press ENTER for next slide. 32
Treatment Plan Objectives Goals should be stated in the positive (e.g., Increase the client’s level of selfesteem). Statements in the positive reinforce the idea that the client is striving to gain something rather than lose something. It is often difficult to attain a positive goal without eliminating or reducing one or more types of behaviors, emotions, or cognitions, it is appropriate to state objectives in the negative. Press ENTER for next slide. 33
Treatment Plan Objectives The goals and objectives should be prioritized. The goals and objectives priority should mirror the priority assigned to the problems. The client can work toward achieving one or more goals at a time. Objectives tied to two or more goals can also be address simultaneously and represents the most efficient use of the client’s and the therapist’s time. Press ENTER for next slide. 34
Treatment Plan Objectives QUESTIONS TO ASK What do you see as your biggest problem? Do you think there is an immediate crisis that needs to be addressed? What do you see as your biggest goal in treatment? How will you know if you have achieved your goal? Does the goal involve changing things about yourself? Does the goal involve changing things about other people? What problems do you anticipate in reaching that goal? How will you be different after reaching the goal? What positive things will you be doing? What negative things will no longer be present? What skills will help you achieve the goal? Press ENTER for next slide. 35
Interventions The plan for how the therapist will assist the client in resolving their problems and consequently achieving their goals and objectives. For clinicians who strictly adhere to a single therapeutic approach (e.g., cognitive-behavioral therapy), the interventions will generally be the same for all clients, regardless of what the problems are. The selection of the intervention to be used becomes more of a challenge for those therapists who are more eclectic in their treatment orientations. Interventions are generally direct interaction with the clinician or other treatment team member and include individual and group interventions. Press ENTER for next slide. 36
Interventions Treatment plans must include the frequency and duration of the intervention. In some instances, statements regarding the frequency and duration may be nothing more than guesses based on the therapist’s experience with similar clients, problems and treatment goals. Open ended treatment durations should be avoided except in cases for which long-term or continuous treatment is appropriate (e.g., schizophrenics or the chronically mentally ill). The therapist should try to provide a very specific and accurate determination of frequency and duration. Press ENTER for next slide. 37
Interventions QUESTIONS TO ASK Will the planned intervention enable to client to meet all or most of the documented goals and objectives? Does the treating therapist have the skills necessary for implementing the planned treatment intervention? Is what the client will be expected to do realistic? Is what the therapist will be expected to do realistic? Will the clinician be able to know within a reasonable amount of time if the intervention is working? Could a different type of intervention yield the same outcome? If so, why was it not selected? Press ENTER for next slide. 38
Criteria for Discharge No treatment plan would be complete without an indication of the criteria for successful discharge from treatment. Must include the Texas Department of Insurance Criteria for discharge from that level of care. The therapist and client must have an agreed upon point at which treatment or a portion of treatment is considered complete and the services being offered to the client are terminated or transferred to a more appropriate LOC. The criteria should be objective and measurable and should reflect the stated goals and objectives. Press ENTER for next slide. 39
Treatment Plan Review There should always be a time indicated for treatment plan review. For residential clients, the treatment plan should be reviewed and updated every 14 days, sooner if there is a significant change in the client’s condition. For outpatient clients, the review should occur every 30 days or sooner if there is a significant change in the client’s condition. Press ENTER for next slide. 40
Progress Note Documentation Press ENTER for next slide. 41
Progress Note Documentation There should be a progress note documented following: each clinical session for each day that the client is present in a residential or detox program at the time of discharge Progress notes must be signed by the author, and have their credentials clearly documented. Progress notes must contain the date of the session and the length of time of the session, with either a beginning and ending time or a total time spent with the client. Progress notes can be written in several different formats. The following are recommended: SOAP DAP Gillman HIPAA Progress Note Press ENTER for next slide. 42
S.O.A.P. Notes S Subjective [client’s view of problems or progress noted, use client’s own words.] O Objective [Therapist’s objective observations of the clients progress.] A Assessment [Therapist’s assessment of the client’s affect, mental status, and psychosocial functioning.] P Plan [Plan for future treatment as it relates to progress noted.] Press ENTER for next slide. 43
D.A.P. Notes D Data [Therapist’s observations, what the clinician saw and heard, quote statements made by the client.] A Assessment [The therapists assessment of the client’s mental status and psychological functioning.] P Plan [Plan for future treatment as it relates to progress noted and updating of the treatment plan.] Press ENTER for next slide. 44
Gillman HIPAA Progress Note This is a new system used to document behavioral therapy notes Created by Peter B. Gillman, PhD, Response to the HIPAA regulations around psychotherapy notes. Press ENTER for next slide. 45
Gillman HIPAA Progress Note The Gillman HIPAA Progress Note contains the following elements: Counseling session start and stop time Modalities of treatment furnished Frequency of modalities furnished Medication prescription and monitoring Results of any clinical tests or assessments Summary of Symptoms Summary of Functional Status Summary of Progress Summary of Diagnosis Summary of Treatment Plan Summary of Progress Press ENTER for next slide. 46
What makes the Gillman HIPAA Note superior to the SOAP or DAP? It requires the clinician to think in more behavioral terms. It requires the clinician to focus on presenting symptoms. It requires the clinician to think about functional environments that the client finds more meaningful to express their psychopathology. It requires the clinician to think about the progress made since the last session. Press ENTER for next slide. 47
What makes the Gillman HIPAA Note superior to the SOAP or DAP?, Cont. It requires the clinician to think about how the above data might change their diagnostic thinking. It requires the clinician to think about changes to their treatment plan and recommendations. It requires the clinician to think about the prognosis until the next treatment session. Press ENTER for next slide. 48
General Considerations Think about what you will write before you write it. Sign and Date every note. Check your notes for grammatical and spelling errors. Limit the use of abbreviations - check with site as to which abbreviations are acceptable. Press ENTER for next slide. 49
General Considerations Errors on hand written notes should have a single line through them, write 'error', initial, and date. Write legibly. Avoid blank spaces between entries. Include client name and case number on each page. Use direct quotations when reporting clinically relevant client quotations. Press ENTER for next slide. 50
General Considerations Describe what was observed not just your opinion about what was observed. Tie notes into your treatment plan goals and objectives. Be as brief as is necessary - that is put enough information down to complete a note well, but don't put more information than is necessary. Clearly note any risk assessment data and contracting. Press ENTER for next slide. 51
General Considerations Remember the chart is a legal document. Because it is a legal document, you should start your note right after the last note in the chart so it will be chronological. For neatness sake you may want to start at the top of a page, so strike out any blank space above your note. You should also provide room for your supervisor to amend your note at the end. Press ENTER for next slide. 52
General Considerations Do not leave blank lines in between text. If you make a mistake, simply cross out the word with a single horizontal line, write “error”, and initial it. Do not scribble/white out a mistake. Press ENTER for next slide. 53






