Children System of Care Application Process for Behavioral Assistance

32 Slides1.26 MB
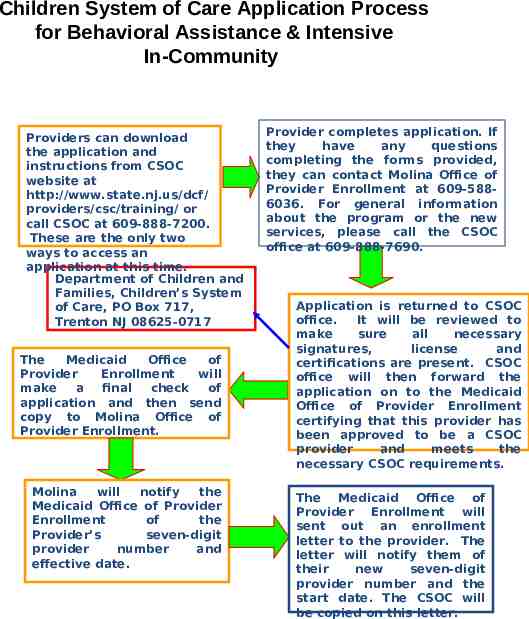
Children System of Care Application Process for Behavioral Assistance & Intensive In-Community Providers can download the application and instructions from CSOC website at http://www.state.nj.us/dcf/ providers/csc/training/ or call CSOC at 609-888-7200. These are the only two ways to access an application at this time. Department of Children and Families, Children’s System of Care, PO Box 717, Trenton NJ 08625-0717 The Medicaid Office of Provider Enrollment will make a final check of application and then send copy to Molina Office of Provider Enrollment. Molina will notify the Medicaid Office of Provider Enrollment of the Provider’s seven-digit provider number and effective date. Provider completes application. If they have any questions completing the forms provided, they can contact Molina Office of Provider Enrollment at 609-5886036. For general information about the program or the new services, please call the CSOC office at 609-888-7690. Application is returned to CSOC office. It will be reviewed to make sure all necessary signatures, license and certifications are present. CSOC office will then forward the application on to the Medicaid Office of Provider Enrollment certifying that this provider has been approved to be a CSOC provider and meets the necessary CSOC requirements. The Medicaid Office of Provider Enrollment will sent out an enrollment letter to the provider. The letter will notify them of their new seven-digit provider number and the start date. The CSOC will be copied on this letter.
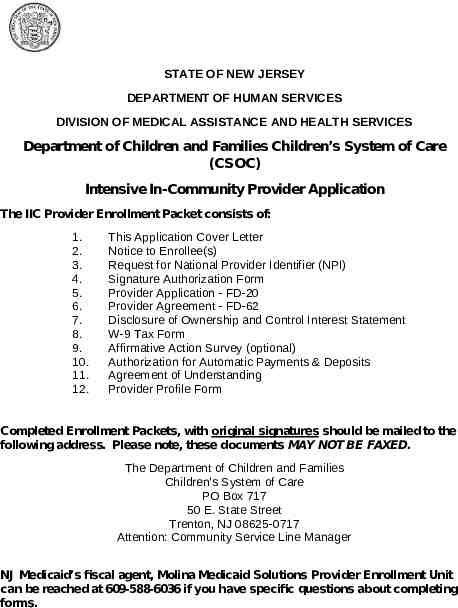
STATE OF NEW JERSEY DEPARTMENT OF HUMAN SERVICES DIVISION OF MEDICAL ASSISTANCE AND HEALTH SERVICES Department of Children and Families Children’s System of Care (CSOC) Intensive In-Community Provider Application The IIC Provider Enrollment Packet consists of: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. This Application Cover Letter Notice to Enrollee(s) Request for National Provider Identifier (NPI) Signature Authorization Form Provider Application - FD-20 Provider Agreement - FD-62 Disclosure of Ownership and Control Interest Statement W-9 Tax Form Affirmative Action Survey (optional) Authorization for Automatic Payments & Deposits Agreement of Understanding Provider Profile Form Completed Enrollment Packets, with original signatures should be mailed to the following address. Please note, these documents MAY NOT BE FAXED. The Department of Children and Families Children’s System of Care PO Box 717 50 E. State Street Trenton, NJ 08625-0717 Attention: Community Service Line Manager NJ Medicaid’s fiscal agent, Molina Medicaid Solutions Provider Enrollment Unit can be reached at 609-588-6036 if you have specific questions about completing forms.
S tateof N ewJ ersey DEPARTMENT OF HUMAN SERVICES DIVISION OF MEDICAL ASSISTANCE AND HEALTH SERVICES CHRIS CHRISTIE Governor P.O. Box 712 Trenton, NJ 08625-0712 Telephone 1-800-356-1561 KIM GUADAGNO Lt. Governor JENNIFER VELEZ Commissioner VALERIE HARR Director Notice to Enrollee(s) In an effort to properly set-up the identity of an individual or an entity as a NJ Medicaid provider the Division requires that when a social security number is the primary means of identity you are required to submit a copy of your social security card. If you are an entity, you are required to submit a copy of your 147C letter from the IRS or copy of the IRS CP-575 form. PLEASE BE ADVISED THAT YOUR APPLICATION TO BECOME A NJ MEDICAID PROVIDER CANNOT BE COMPLETED UNTIL WE HAVE RECEIVED A COPY OF THESE DOCUMENTS.
Request for National Provider Identifier (NPI) The Center for Medicare & Medicaid Services (CMS) established a May 23, 2007 deadline for implementing NPI provisions. On April 2, 2007, CMS extended the deadline to May 23, 2008. However, it is the intention of the State of New Jersey to establish a Statewide Deadline for requiring compliance with all NPI provisions as of January 1, 2013. The Division of Medical Assistance & Health Services (DMAHS), in cooperation with other State agencies, will notify providers regarding the Statewide Deadline for compliance with NPI provisions when transmitting a health care claim for payment as a standard electronic HIPAA transaction or paper claim. All health care providers can apply for an NPI: Using the web-based application https://nppes.cms.hhs.gov; or Sending a paper application to the Center for Medicare & Medicaid Services’ (CMS’) NPI Enumerator, Fox Systems. A copy of the application can be downloaded at https://nppes.cms.hhs.gov. A health care provider can also contact the Enumerator at 1-800-4653203 or TTY 1-800-692-2326. You application cannot be processed until you have an NPI.
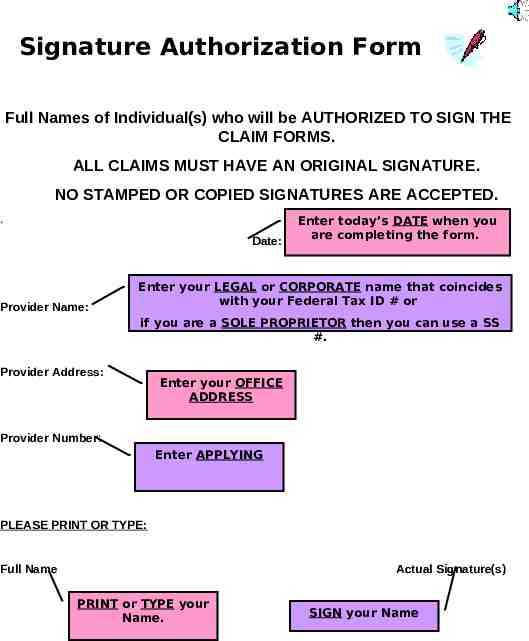
Signature Authorization Form Full Names of Individual(s) who will be AUTHORIZED TO SIGN THE CLAIM FORMS. ALL CLAIMS MUST HAVE AN ORIGINAL SIGNATURE. NO STAMPED OR COPIED SIGNATURES ARE ACCEPTED. . Date: Provider Name: Enter today’s DATE when you are completing the form. Enter your LEGAL or CORPORATE name that coincides with your Federal Tax ID # or if you are a SOLE PROPRIETOR then you can use a SS #. Provider Address: Enter your OFFICE ADDRESS Provider Number: Enter APPLYING PLEASE PRINT OR TYPE: Full Name Actual Signature(s) PRINT or TYPE your Name. SIGN your Name
Signature Authorization Form Dear Provider: Please furnish below the full names of those individuals you have authorized to sign and certify Medicaid claims and supporting documents. If the authorized individual is the Medicaid Provider, he/she must sign the Authorization Form. In addition to the above, this form should only be completed by an authorized representative(s) who is an employee of your office. Should your office utilize a billing firm or agency, a letter signed by yourself must be submitted indicating the name(s) of those individuals you have authorized to sign. The name(s) should be typed and then the actual signature affixed by that individual. The letter should contain the name of the billing firm or agency which has been approved to provide your billing. Date: Provider Name Provider Address Provider Number PLEASE PRINT OR TYPE: Full Name Actual Signature(s)
FD-20 Application
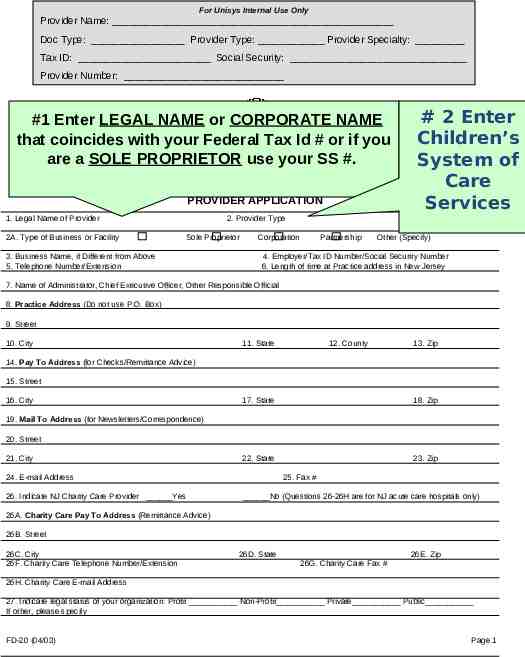
FD-20 Application #1. Enter LEGAL NAME or CORPORATE NAME that coincides with your Federal Tax Id # or if you are a SOLE PROPRIETOR use your SS #. #2. Enter Children’s System of Care Services. #3. Enter the NAME OF YOUR BUSINESS, if different then # 1 (legal name). i.e. What is your business called?
FD 20 Application, cont’d #4. Employer Tax Id #: 9digits given by the IRS @ start of your business. #5. Telephone # & Extension: A # where you can be outreached. #8-13. Practice Office: Location of actual business. #14-18. Pay Address: Where Checks & Remittance Advices (RA’s) are mailed.
FD 20 Application, cont’d #19-23. Mail Address: Where Newsletters/Correspondenc e are mailed. #24. E-mail Address. #25. Fax #. #28. Indicate Type of Service: Behavior Assistance, Intensive InCommunity or Both.
FD 20 Application, cont’d #29. List All Offices within that county. #35. List Name(s) & Degree(s) as appropriate & submit Copy of Current License(s). 37. Check “All” & List usual & customary Fees.
For Unisys Internal Use Only Provider Name: Doc Type: Provider Type: Provider Specialty: Tax ID: Social Security: Provider Number: #1 Enter LEGAL NAME or CORPORATE NAME that coincides with your State Federal Tax Id # or if you of New Jersey are a SOLE PROPRIETOR your SS #. DEPARTMENT OFuse HUMAN SERVICES Division of Medical Assistance and Health Services PROVIDER APPLICATION 1. Legal Name of Provider 2A. Type of Business or Facility # 2 Enter Children’s System of Care Services 2. Provider Type Sole Proprietor 3. Business Name, if Different from Above 5. Telephone Number/Extension Corporation Partnership Other (Specify) 4. Employer/Tax ID Number/Social Security Number 6. Length of time at Practice address in New Jersey 7. Name of Administrator, Chief Executive Officer, Other Responsible Official 8. Practice Address (Do not use P.O. Box) 9. Street 10. City 11. State 12. County 13. Zip 14. Pay To Address (for Checks/Remittance Advice) 15. Street 16. City 17. State 18. Zip 22. State 23. Zip 19. Mail To Address (for Newsletters/Correspondence) 20. Street 21. City 24. E-mail Address 26. Indicate NJ Charity Care Provider Yes 25. Fax # No (Questions 26-26H are for NJ acute care hospitals only) 26A. Charity Care Pay To Address (Remittance Advice) 26B. Street 26C. City 26F. Charity Care Telephone Number/Extension 26D. State 26E. Zip 26G. Charity Care Fax # 26H. Charity Care E-mail Address 27. Indicate legal status of your organization: Profit Non-Profit Private Public If other, please specify FD-20 (04/03) Page 1
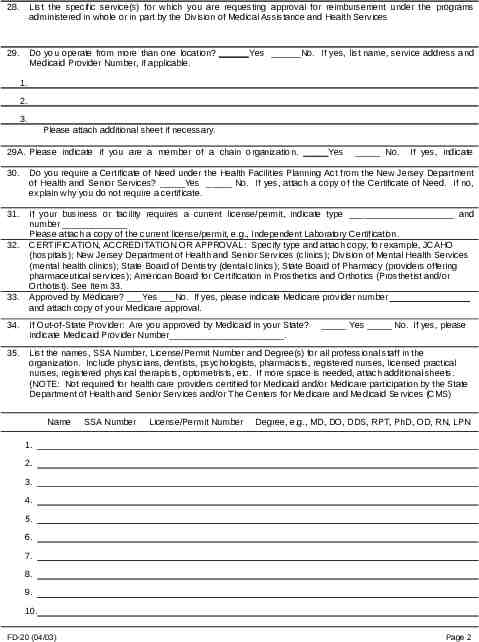
28. List the specific service(s) for which you are requesting approval for reimbursement under the programs administered in whole or in part by the Division of Medical Assistance and Health Services 29. Do you operate from more than one location? Yes No. If yes, list name, service address and Medicaid Provider Number, if applicable. 1. 2. 3. Please attach additional sheet if necessary. 29A. Please indicate if you are a member of a chain organization. Yes No. If yes, indicate name 30. Do you require a Certificate of Need under the Health Facilities Planning Act from the New Jersey Department of Health and Senior Services? Yes No. If yes, attach a copy of the Certificate of Need. If no, explain why you do not require a certificate. 31. 32. 33. If your business or facility requires a current license/permit, indicate type and number Please attach a copy of the current license/permit, e.g., Independent Laboratory Certification. CERTIFICATION, ACCREDITATION OR APPROVAL: Specify type and attach copy, for example, JCAHO (hospitals); New Jersey Department of Health and Senior Services (clinics); Division of Mental Health Services (mental health clinics); State Board of Dentistry (dental clinics); State Board of Pharmacy (providers offering pharmaceutical services); American Board for Certification in Prosthetics and Orthotics (Prosthetist and/or Orthotist). See Item 33. Approved by Medicare? Yes No. If yes, please indicate Medicare provider number and attach copy of your Medicare approval. 34. If Out-of-State Provider: Are you approved by Medicaid in your State? indicate Medicaid Provider Number . 35. List the names, SSA Number, License/Permit Number and Degree(s) for all professional staff in the organization. Include physicians, dentists, psychologists, pharmacists, registered nurses, licensed practical nurses, registered physical therapists, optometrists, etc. If more space is needed, attach additional sheets. (NOTE: Not required for health care providers certified for Medicaid and/or Medicare participation by the State Department of Health and Senior Services and/or The Centers for Medicare and Medicaid Services (CMS) Name SSA Number License/Permit Number Yes No. If yes, please Degree, e.g., MD, DO, DDS, RPT, PhD, OD, RN, LPN 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. FD-20 (04/03) Page 2
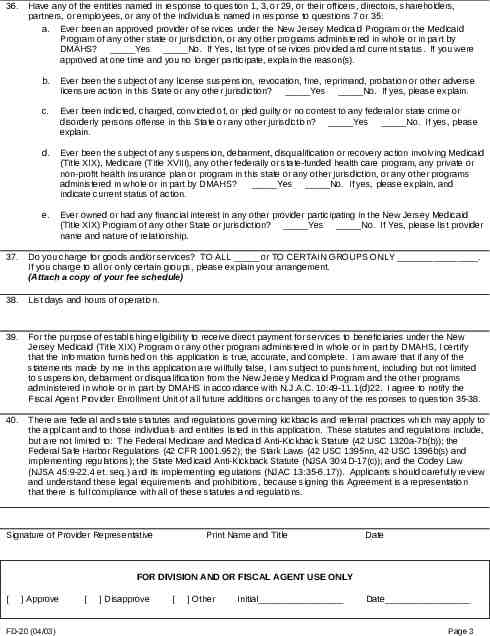
36. Have any of the entities named in response to question 1, 3, or 29, or their officers, directors, shareholders, partners, or employees, or any of the individuals named in response to questions 7 or 35: a. Ever been an approved provider of services under the New Jersey Medicaid Program or the Medicaid Program of any other state or jurisdiction, or any other programs administered in whole or in part by DMAHS? Yes No. If Yes, list type of services provided and current status. If you were approved at one time and you no longer participate, explain the reason(s). b. Ever been the subject of any license suspension, revocation, fine, reprimand, probation or other adverse licensure action in this State or any other jurisdiction? Yes No. If yes, please explain. c. Ever been indicted, charged, convicted of, or pled guilty or no contest to any federal or state crime or disorderly persons offense in this State or any other jurisdiction? Yes No. If yes, please explain. d. Ever been the subject of any suspension, debarment, disqualification or recovery action involving Medicaid (Title XIX), Medicare (Title XVIII), any other federally or state-funded health care program, any private or non-profit health insurance plan or program in this state or any other jurisdiction, or any other programs administered in whole or in part by DMAHS? Yes No. If yes, please explain, and indicate current status of action. e. Ever owned or had any financial interest in any other provider participating in the New Jersey Medicaid (Title XIX) Program of any other State or jurisdiction? Yes No. If Yes, please list provider name and nature of relationship. 37. Do you charge for goods and/or services? TO ALL or TO CERTAIN GROUPS ONLY . If you charge to all or only certain groups, please explain your arrangement. (Attach a copy of your fee schedule) 38. List days and hours of operation. 39. For the purpose of establishing eligibility to receive direct payment for services to beneficiaries under the New Jersey Medicaid (Title XIX) Program or any other program administered in whole or in part by DMAHS, I certify that the information furnished on this application is true, accurate, and complete. I am aware that if any of the statements made by me in this application are willfully false, I am subject to punishment, including but not limited to suspension, debarment or disqualification from the New Jersey Medicaid Program and the other programs administered in whole or in part by DMAHS in accordance with N.J.A.C. 10:49-11.1(d)22. I agree to notify the Fiscal Agent Provider Enrollment Unit of all future additions or changes to any of the responses to question 35-38. 40. There are federal and state statutes and regulations governing kickbacks and referral practices which may apply to the applicant and to those individuals and entities listed in this application. These statutes and regulations include, but are not limited to: The Federal Medicare and Medicaid Anti-Kickback Statute (42 USC 1320a-7b(b)); the Federal Safe Harbor Regulations (42 CFR 1001.952); the Stark Laws (42 USC 1395nn, 42 USC 1396b(s) and implementing regulations); the State Medicaid Anti-Kickback Statute (NJSA 30:4D-17(c)); and the Codey Law (NJSA 45:9-22.4 et. seq.) and its implementing regulations (NJAC 13:35-6.17)). Applicants should carefully review and understand these legal requirements and prohibitions, because signing this Agreement is a representation that there is full compliance with all of these statutes and regulations. Signature of Provider Representative Print Name and Title Date FOR DIVISION AND OR FISCAL AGENT USE ONLY [ ] Approve FD-20 (04/03) [ ] Disapprove [ ] Other Initial Date Page 3
Provider Agreement FD-62
FD-62 Agreeing to: All Terms & Conditions Comply w/ all State & Federal Laws Maintain Medical Record Furnish Info. re: Payments Claimed for Services Comply w/ all Amendments which makes it a Crime for persons making any False Statements or Representations Accept Payment as Payment in Full & not to Institute Collection Activities against Beneficiaries
This document outlines STATE O F N EW JER SEY D E P A R T M E N T O Fare H U M A N Sagreeing E R V IC E S what you to D IV IS IO N O F M E D IC A L A S S IS T A N C E A N D H E A L T H S E R V IC E S R O V ID ECSOC R A G R E E M E N TMedicaid as a PNJ B E TW E E N N E W J E R S E Y D IV IS IO N O F M E D IC A L A S S IS T A N C E A N D H E A L T H S E R V IC E S Provider AN D P R O V ID E R N A M E P R O V ID E R A G R E E S : 1 . T o c o m p ly w ith a ll a p p lic a b le S ta te a n d F e d e ra l la w s, p o lic ie s , ru le s a n d re g u la tio n s p rom u lg ate d p u rs u a n t th e re to; 2 . T o ke e p s u ch re c ord s a s a re n e c e s s a ry to fu lly d is c lo s e th e e xte n t of se rvic e s p ro vid e d to in d ivid u a ls re c e ivin g a ss is ta n ce u n d er th e [M e d ic a id ] p ro g ra m s a d m in is te re d in w h o le o r in p a rt b y th e D iv is io n o f M e d ic a id A ss ista n c e a n d H e a lth S e rvic e s (D M A H S ), a n d to p ro vid e a n y a u th o rize d D M A H S e m p lo ye e o r a g e n t w ith c o p ie s o f re q u e s te d re c o rd s fre e o f a ll c o p y fe e s a n d re la te d d u p lic a tio n c h a rg e s; 3 . T o fu rn is h th e D M A H S , th e S e c reta ry o f th e U .S . D e p a rtm e n t o f H e a lth a n d H u m a n S e rvic e s a n d th e M e d ic a id F ra u d S e ctio n o f th e D ivis io n o f C rim in a l J u stic e w ith s u c h in fo rm a tio n a s m a y b e re q u e s te d from tim e to tim e , re g a rd in g a n y p aym e n ts cla im e d fo r p ro vid in g s e rvic e s u n d e r th e p ro g ra m s a d m in is te re d in w h o le o r in p a rt b y D M A H S ; 4 . T o co m p ly w ith th e re q u ire m e n ts o f T itle V I o f the C ivil R ig h ts A c ts o f 1 96 4 a n d S e c tio n 5 0 4 o f the R e h a b ilita tio n A c t of 1 9 73 a n d a n y a m e n d m e nts th e re to ; a n d S e ctio n 1 9 0 9 of P .L . 9 2 -6 0 3, S e ctio n 2 4 2 8 w h ic h m a k e s it a c rim e a n d s e ts th e p u n ish m e n t fo r p e rs o n s w h o h a ve b e e n fo u n d g u ilty of m ak in g a n y fa lse s ta te m e n t o r re p re s e n ta tio n of a m a te ria l fa c t in o rd e r to re c e i ve a n y b e n e fit o r p a ym e n t u n d e r th e M e d ica l A ss is ta n c e P ro g ram . (T h e D e p a rtm e n t o f H u m a n S e rvic e s is re q u ired b y F e d e ra l re g u latio n to m a k e th is la w k n o w n a n d to w a rn a g a in s t fa ls e sta tem e n ts in an a p p lic a tio n / a g re e m e n t o r in a fa c t u se d in d e te rm in in g t h e rig h t to a b e n efit, o r c o n ve rtin g a b e n efit to th e u s e of a n y p e rs o n o th e r th a n o n e fo r w h o m it w a s in te n d e d ). Must Sign & Date Print Name & Title 5 . T o c o m p ly w ith th e d is clo su re re q u ire m en ts s p e cifie d in 4 2 C F R 4 5 5 .1 0 0 th ro ug h 4 2 C F R 4 5 5 .1 0 6 . 6 . T o ac c e p t T itle X IX p a ym e n ts a s p a ym e nt in fu ll, a n d n o t in stitu te c o lle c tio n a ctivitie s, in c lu d in g bu t lim ite d to , b illin g , b a la n ce b illin g a n d litig a tio n, a g a in st T itle X IX b e n e fic ia rie s fo r th e p a ym e n t of c la im s th a t h a ve b e e n d e n ie d in w h o le o r in p a rt b y D M A H S o r its fis c a l a g e n t, e xc e p t a s p e rm itte d b y N J S A 3 0 :4 D -6 .c., o r o th e rw is e p e rm itte d o r req u ire d b y S ta te o r F e d e ra l L a w . T h e pro vid e r o r D M A H S m a y, o n 6 0 d a ys w ritte n n o tic e to th e D ivis io n , term in a te th is A g ree m e n t w ith o u t ca u s e . DATE S IG N A T U R E O F P R O V ID E R P R IN T N A M E A N D T IT LE F D -6 2 (R E V 1 2 /0 2 ) M e d ic a id 3 0 3 1 -M E d 6 /86
Ownership & Control Interest Statement Any entity, corporation or facility – this form is utilized to indicate any type of controlling ownership that exists w/in your facility. Any change of ownership – a NEW form must be completed & submitted.
Ownership & Control Interest Statement Required Fields Section 1 #1. Name of Entity #2. Telephone # #3. Street Address, City, County, State & Zip Code Section 2 All Question. Yes, No or N/A. Section 3 Only required if you are an individual w/ a direct or indirect ownership. Section 4 thru Section 8 All Questions. Yes, No or N/A. Last Section Print Name of Authorized Representative & Title w/ Signature & Date.
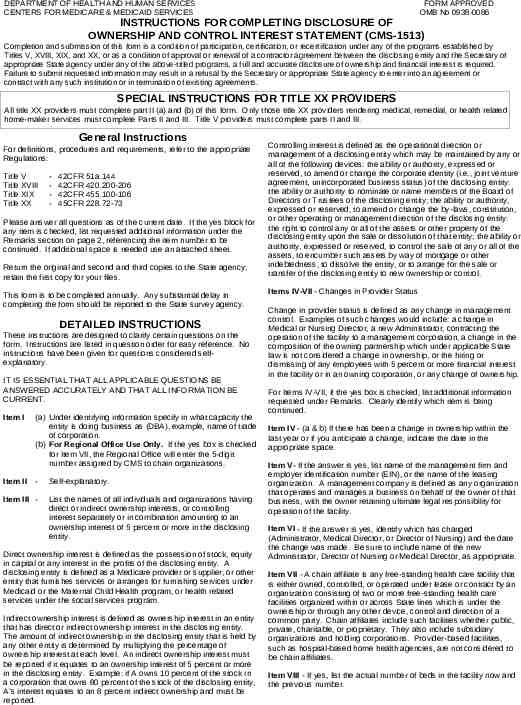
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES FORM APPROVED OMB No 0938-0086 INSTRUCTIONS FOR COMPLETING DISCLOSURE OF OWNERSHIP AND CONTROL INTEREST STATEMENT (CMS-1513) Completion and submission of this form is a condition of participation, certification, or recertification under any of the programs established by Titles V, XVIII, XIX, and XX, or as a condition of approval or renewal of a contractor agreement between the disclosing entity and the Secretary of appropriate State agency under any of the above-titled programs, a full and accurate disclosure of ownership and financial interest is required. Failure to submit requested information may result in a refusal by the Secretary or appropriate State agency to enter into an agreement or contract with any such institution or in termination of existing agreements. SPECIAL INSTRUCTIONS FOR TITLE XX PROVIDERS All title XX providers must complete part II (a) and (b) of this form. Only those title XX providers rendering medical, remedial, or health related home-maker services must complete Parts II and III. Title V providers must complete parts II and III. General Instructions For definitions, procedures and requirements, refer to the appropriate Regulations: Title V Title XVIII Title XIX Title XX - 42CFR 51a.144 42CFR 420.200-206 42CFR 455.100-106 45CFR 228.72-73 Please answer all questions as of the current date. If the yes block for any item is checked, list requested additional information under the Remarks section on page 2, referencing the item number to be continued. If additional space is needed use an attached sheet. Return the original and second and third copies to the State agency; retain the first copy for your files. This form is to be completed annually. Any substantial delay in completing the form should be reported to the State survey agency. DETAILED INSTRUCTIONS These instructions are designed to clarify certain questions on the form. Instructions are listed in question order for easy reference. No instructions have been given for questions considered selfexplanatory. IT IS ESSENTIAL THAT ALL APPLICABLE QUESTIONS BE ANSWERED ACCURATELY AND THAT ALL INFORMATION BE CURRENT. Item I Item II (a) Under identifying information specify in what capacity the entity is doing business as (DBA), example, name of trade of corporation. (b) For Regional Office Use Only. If the yes box is checked for Item VII, the Regional Office will enter the 5-digit number assigned by CMS to chain organizations. - Item III - Self-explanatory. List the names of all individuals and organizations having direct or indirect ownership interests, or controlling interest separately or in combination amounting to an ownership interest of 5 percent or more in the disclosing entity. Direct ownership interest is defined as the possession of stock, equity in capital or any interest in the profits of the disclosing entity. A disclosing entity is defined as a Medicare provider or supplier, or other entity that furnishes services or arranges for furnishing services under Medicaid or the Maternal Child Health program, or health related services under the social services program. Indirect ownership interest is defined as ownership interest in an entity that has direct or indirect ownership interest in the disclosing entity. The amount of indirect ownership in the disclosing entity that is held by any other entity is determined by multiplying the percentage of ownership interest at each level. An indirect ownership interest must be reported if it equates to an ownership interest of 5 percent or more in the disclosing entity. Example: if A owns 10 percent of the stock in a corporation that owns 80 percent of the stock of the disclosing entity, A’s interest equates to an 8 percent indirect ownership and must be reported. Controlling interest is defined as the operational direction or management of a disclosing entity which may be maintained by any or all of the following devices: the ability or authority, expressed or reserved, to amend or change the corporate identity (i.e., joint venture agreement, unincorporated business status) of the disclosing entity: the ability or authority to nominate or name members of the Board of Directors or Trustees of the disclosing entity; the ability or authority, expressed or reserved, to amend or change the by-laws, constitution, or other operating or management direction of the disclosing entity: the right to control any or all of the assets or other property of the disclosing entity upon the sale or dissolution of that entity; the ability or authority, expressed or reserved, to control the sale of any or all of the assets, to encumber such assets by way of mortgage or other indebtedness, to dissolve the entity, or to arrange for the sale or transfer of the disclosing entity to new ownership or control. Items IV-VII - Changes in Provider Status Change in provider status is defined as any change in management control. Examples of such changes would include: a change in Medical or Nursing Director, a new Administrator, contracting the operation of the facility to a management corporation, a change in the composition of the owning partnership which under applicable State law is not considered a change in ownership, or the hiring or dismissing of any employees with 5 percent or more financial interest in the facility or in an owning corporation, or any change of ownership. For Items IV-VII, if the yes box is checked, list additional information requested under Remarks. Clearly identify which item is being continued. Item IV - (a & b) If there has been a change in ownership within the last year or if you anticipate a change, indicate the date in the appropriate space. Item V- If the answer is yes, list name of the management firm and employer identification number (EIN), or the name of the leasing organization. A management company is defined as any organization that operates and manages a business on behalf of the owner of that business, with the owner retaining ultimate legal responsibility for operation of the facility. Item VI - If the answer is yes, identify which has changed (Administrator, Medical Director, or Director of Nursing) and the date the change was made. Be sure to include name of the new Administrator, Director of Nursing or Medical Director, as appropriate. Item VII - A chain affiliate is any free-standing health care facility that is either owned, controlled, or operated under lease or contract by an organization consisting of two or more free-standing health care facilities organized within or across State lines which is under the ownership or through any other device, control and direction of a common party. Chain affiliates include such facilities whether public, private, charitable, or proprietary. They also include subsidiary organizations and holding corporations. Provider-based facilities, such as hospital-based home health agencies, are not considered to be chain affiliates. Item VIII - If yes, list the actual number of beds in the facility now and the previous number.
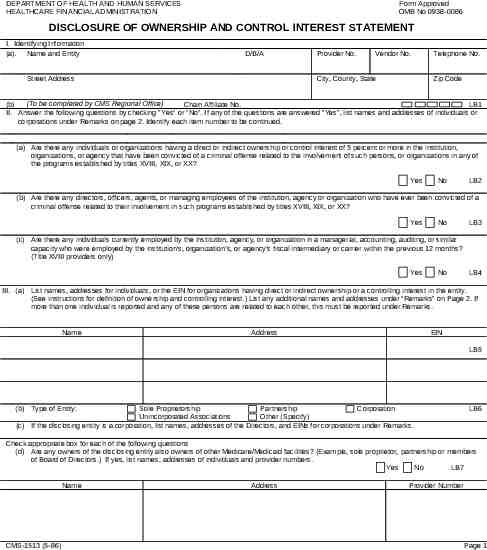
DEPARTMENT OF HEALTH AND HUMAN SERVICES HEALTHCARE FINANCIAL ADMINISTRATION Form Approved OMB No 0938-0086 DISCLOSURE OF OWNERSHIP AND CONTROL INTEREST STATEMENT I. Identifying Information (a). Name and Entity D/B/A Street Address Provider No. Vendor No. City, County, State Telephone No. Zip Code (To be completed by CMS Regional Office) (b) Chain Affiliate No. LB1 II. Answer the following questions by checking "Yes" or "No". If any of the questions are answered “Yes”, list names and addresses of individuals or corporations under Remarks on page 2. Identify each item number to be continued. (a) Are there any individuals or organizations having a direct or indirect ownership or control interest of 5 percent or more in the institution, organizations, or agency that have been convicted of a criminal offense related to the involvement of such persons, or organizations in any of the programs established by titles XVIII, XIX, or XX? Yes No LB2 (b) Are there any directors, officers, agents, or managing employees of the institution, agency or organization who have ever been convicted of a criminal offense related to their involvement in such programs established by titles XVIII, XIX, or XX? Yes No LB3 (c) Are there any individuals currently employed by the institution, agency, or organization in a managerial, accounting, auditing, or similar capacity who were employed by the institution's, organization’s, or agency’s fiscal intermediary or carrier within the previous 12 months? (Title XVIII providers only) Yes No LB4 III. (a) List names, addresses for individuals, or the EIN for organizations having direct or indirect ownership or a controlling interest in the entity. (See instructions for definition of ownership and controlling interest.) List any additional names and addresses under “Remarks" on Page 2. If more than one individual is reported and any of these persons are related to each other, this must be reported under Remarks. Name Address EIN LB5 (b) Type of Entity: Sole Proprietorship Partnership Corporation Unincorporated Associations Other (Specify) (c) If the disclosing entity is a corporation, list names, addresses of the Directors, and EINs for corporations under Remarks. LB6 Check appropriate box for each of the following questions (d) Are any owners of the disclosing entity also owners of other Medicare/Medicaid facilities? (Example, sole proprietor, partnership or members of Board of Directors.) If yes, list names, addresses of individuals and provider numbers. Yes No LB7 Name CMS-1513 (5-86) Address Provider Number Page 1
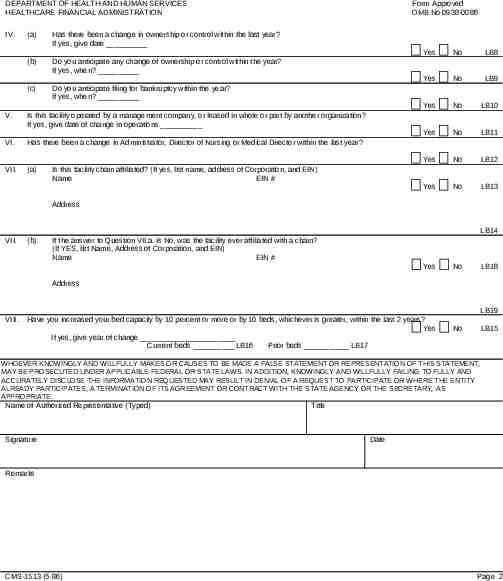
DEPARTMENT OF HEALTH AND HUMAN SERVICES HEALTHCARE FINANCIAL ADMINISTRATION IV. (a) Has there been a change in ownership or control within the last year? If yes, give date (b) Do you anticipate any change of ownership or control within the year? If yes, when? (c) Do you anticipate filing for bankruptcy within the year? If yes, when? Form Approved OMB No 0938-0086 V. Is this facility operated by a management company, or leased in whole or part by another organization? If yes, give date of change in operations VI. Has there been a change in Administrator, Director of Nursing or Medical Director within the last year? VII. (a) Yes No LB8 Yes No LB9 Yes No LB10 Yes No LB11 Yes No LB12 Yes No LB13 Is this facility chain affiliated? (If yes, list name, address of Corporation, and EIN) Name EIN # Address LB14 VII. (b) If the answer to Question VII.a. is No, was the facility ever affiliated with a chain? (If YES, list Name, Address of Corporation, and EIN) Name EIN # Yes No LB18 Address LB19 VIII. Have you increased your bed capacity by 10 percent or more or by 10 beds, whichever is greater, within the last 2 years? Yes If yes, give year of change Current beds LB16 Prior beds LB17 No LB15 WHOEVER KNOWINGLY AND WILLFULLY MAKES OR CAUSES TO BE MADE A FALSE STATEMENT OR REPRESENTATION OF THIS STATEMENT, MAY BE PROSECUTED UNDER APPLICABLE FEDERAL OR STATE LAWS. IN ADDITION, KNOWINGLY AND WILLFULLY FAILING TO FULLY AND ACCURATELY DISCLOSE THE INFORMATION REQUESTED MAY RESULT IN DENIAL OF A REQUEST TO PARTICIPATE OR WHERE THE ENTITY ALREADY PARTICIPATES, A TERMINATION OF ITS AGREEMENT OR CONTRACT WITH THE STATE AGENCY OR THE SECRETARY, AS APPROPRIATE. Name of Authorized Representative (Typed) Signature Title Date Remarks CMS-1513 (5-86) Page 2
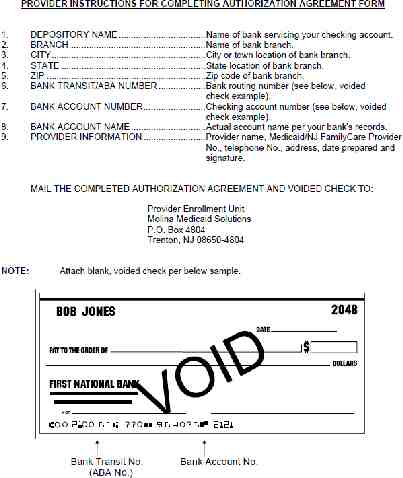
S tateof N ewJ ersey DEPARTMENT OF HUMAN SERVICES DIVISION OF MEDICAL ASSISTANCE AND HEALTH SERVICES CHRIS CHRISTIE Governor P.O. Box 712 Trenton, NJ 08625-0712 Telephone 1-800-356-1561 KIM GUADAGNO Lt. Governor JENNIFER VELEZ Commissioner VALERIE HARR Director *Agreement of Understanding To the Person Submitting this Enrollment Packet: I understand that upon receipt of this enrollment packet to Molina Medicaid Solutions, it becomes property of the State of New Jersey. The enrollment packet and any documents that are generated as result of the submission of this application, such as but not limited to, an enrollment letter or a denial letter are subjected to the Open Public Records Act (OPRA see NJSA Section 47:1A). Before any documents are sent to someone requesting this information, all personal information such as tax Id and social security numbers would be redacted. It is the responsibility of the person signing this Agreement of Understanding to convey this information to all of individuals who are named in this application to become a New Jersey Medicaid provider. Although the request for enrollment information is uncommon, it does fall under the Open Public Records Act. I have read this Agreement of Understanding and acknowledge that once I submit these documents for processing that they will become property of the State of New Jersey. Sign Print Name of Entity or Enrollee, NPI Number and Tax ID Number Date *A signed Agreement of Understanding is required before an application can be processed. Rev: 03/6/2012
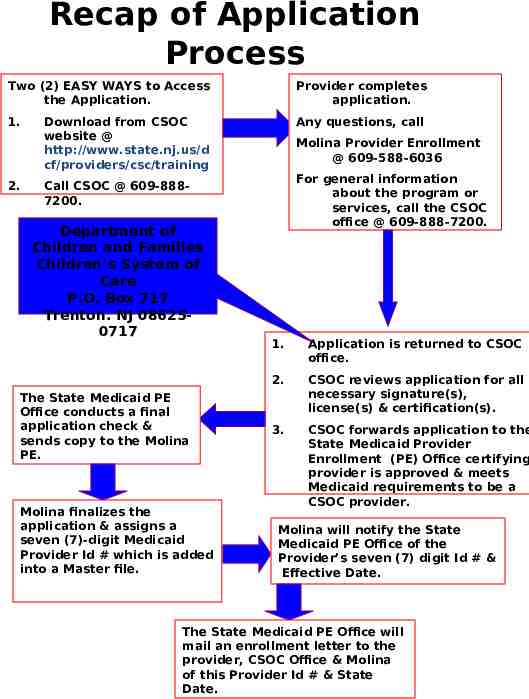
Recap of Application Process Two (2) EASY WAYS to Access the Application. Provider completes application. 1. Any questions, call 2. Download from CSOC website @ http://www.state.nj.us/d cf/providers/csc/training Molina Provider Enrollment @ 609-588-6036 For general information about the program or services, call the CSOC office @ 609-888-7200. Call CSOC @ 609-8887200. Department of Children and Families Children’s System of Care P.O. Box 717 Trenton. NJ 086250717 The State Medicaid PE Office conducts a final application check & sends copy to the Molina PE. Molina finalizes the application & assigns a seven (7)-digit Medicaid Provider Id # which is added into a Master file. 1. Application is returned to CSOC office. 2. CSOC reviews application for all necessary signature(s), license(s) & certification(s). 3. CSOC forwards application to the State Medicaid Provider Enrollment (PE) Office certifying provider is approved & meets Medicaid requirements to be a CSOC provider. Molina will notify the State Medicaid PE Office of the Provider’s seven (7) digit Id # & Effective Date. The State Medicaid PE Office will mail an enrollment letter to the provider, CSOC Office & Molina of this Provider Id # & State Date.
Web Site Information Download Application visit CSOC @ http://www.state.nj.us/dcf/provider s/csc/training General Information about Medicaid Provider Inquiries & Questions visit www.njmmis.com
Who to call for Help? (when completing the application) (general information or new services ) General Information about the Program or New Services, call CSOC @ 609-8887200. Molina Provide Enrollment Office @ 609-588-6036.
Open for Questions