2017 QHP Certification















































63 Slides527.82 KB
2017 QHP Certification
Nevada SBM-FP Notes (Nevada is considered a State Based Marketplace – Federal Platform) QHP Submission through SERFF QHP Approval/Certification for on exchange plans by the Exchange QHP Display on Healthcare.gov QHP/APTC/CSR eligibility determined by Federal guidelines Medicaid/CHIP eligibility determined by State of Nevada DWSS QHP Billing is performed by carriers
QHP Certification Process QHP application in the form of a SERFF binder is required by 5/2 (Incomplete/partial binders and templates will not be accepted per CMS) URRT must be submitted in both HIOS and within SERFF as a supporting document Attestations will be collected from carriers following final data transfer to CMS in August A QHP Issuer Agreement for the 2017 benefit year will need to be signed at the end of the certification process
5/2 5/4 5/20 6/1 6/15 6/20 6/24 7/8 8/12 8/17 11/1 QHP Timeline Key Dates All QHP rate, form and binder filings due in SERFF 1st SERFF data transfer to CMS Correction notices sent to carriers via SERFF Revised data submitted to SERFF Correction notices sent to carriers Revised data submitted to SERFF Second SERFF data transfer to CMS Correction notices sent to carriers via SERFF Final date for carriers to resubmit data Final data transfer from SERFF to CMS Open enrollment
Required Templates (Use latest 2017 templates) ECP/Network Adequacy Template Plans and Benefits Template (and Add-in file) Prescription Drug Formulary Template Network Template Service Area Template Rates Table Template Business Rules Template Administrative Data Template (use 2016 template, add to Supporting Documents section)
Key Changes to Plans and Benefits Template (Benefits Package Worksheet) Standardized Plan Design Add-in File Minimum Stay and State-Required Benefit removed EHB Variance Reason Above EHB changed to Not EHB New field, Design Type, which allows you to indicate whether the plan will follow a standardized plan design. The fields that make up the AV Calculator Additional Benefits section have been moved to CSV Worksheet. (Maximum Coinsurance for Specialty Drugs, Maximum Number of Days for Charging an Inpatient Copay?, Begin Primary Care Cost-Sharing After a Set Number of Visits?, and Begin Primary Care Deductible/Coinsurance After a Set Number of Copays? )
Key Changes to Plans and Benefits Template (Cost Share Variances Worksheet) Check AV Calc macro will provide an option to save an Excel file instance of AVC New SBC scenario for Treatment of a Simple Fracture Field, EHB Apportionment for Pediatric Dental should be a percentage Copay and Coinsurance may include up to two decimal places The Plan Marketing Name has been renamed Plan Variant Marketing Name and can be edited for each plan variation
Standardized Plans Standardized plan designs are optional, and not required for PY2017 In the 2017 Payment Notice Final Rule, it finalized standardized options for bronze, silver (and CSR levels), and gold metal levels Issuers have the option to offer standardized plans at one metal level of coverage and not the others, unless it is silver then must have standardized silver cost-sharing levels.
Tips for Plans and Benefits Template EHB Percent of Premium must match value in URR Template (EHB % might not always be 100% if benefits are greater than minimum) Design Type (new field, which indicates if plan will follow a standardized plan design) URLs for Enrollment Payment, SBC, Plan Brochure are required
Required Fields for Business Rules Template Required minimum relationships between primary and dependent: Spouse-no, Adopted Child-no, Foster Child-no, Ward-no, Stepson or Stepdaughter-no, Self-yes, Child-no, Life Partner-no, Other Relationship-no* *Other Relationship is required for SHOP plans, and if also selling individual plans it must be added because the relationships have to be identical
Application Tips and Hints Plans and Benefits Template Each product should be its own benefit package in the template. QHP/Non-QHP – must select both because of guaranteed availability. For specialties, if there is a “yes” in “specialist requiring a referral,” the next field should also be populated, most of the time with “ALL.” Individual plan’s expiration date: Should always be 12/31/2017. (Not applicable to SHOP) Actual URL for payment information must be working by 8/15
Application Tips and Hints (cont) Plans and Benefits Template (cont) On the cost sharing tab of the template, verify the following do not apply for silver plans: Deductible does not increase as actuarial values increase. MOOP does not increase as the actuarial values increase. Cost sharing for all benefits does not increase as the actuarial values increase. On the cost sharing tab of the template, verify the following do not apply for any cost sharing plan variations: You have listed a non-zero cost sharing for an essential health benefit. The zero cost sharing plan has values of zero for deductible and MOOP.
Application Tips and Hints (cont) Accreditation All issuers applying for 2nd or later year of certification must be accredited by one of the HHS recognized accrediting entities (NCQA, URAC, AAAHC) Verify that all products on Accreditation Template do not expire before November 1, 2016. Must do Attestation in addition to Accreditation Template. Indian Health Care Providers Addendum Issuers are required to offer contracts in good faith to Indian Health Care Providers. There are some provisions pertaining to Indian health care providers that are not applicable to regular QHP/Network Provider agreement. These provisions are addressed in the document called “Model QHP Addendum for Indian Health Care Providers.” Issuers who do contract with Indian Health Providers must sign the Addendum. The Indian Health Care Provider must also sign. The terms in the Addendum will supersede terms in regular QHP/Network Provider contract.
Application Tips and Hints (Cont) Administrative With the elimination of the Administrative Data Template, information must be entered directly into HIOS. The HIOS data is used to populate HealthCare.gov. (Also submit the 2016 template of Administrative Data Template into supporting documents) Unified Rate Review Verify list of plan IDs entered on URRT and Plans and Benefits template match exactly.
Application Tips and Hints (cont) Plan Crosswalk Include all plans that were offered on the Marketplace in 2016, including those that were suppressed following open enrollment if they received enrollees. Don’t need to include withdrawn plans. File name for automatically created XML file must not be changed. When entering the Reason for Crosswalk, only select the “Discontinuing Product” reasons if you are not offering any plans in that product in any counties for the 2017 plan year.
Required Supporting Documentation and Other Tasks ECP Supplemental Response Form Statement of Detailed Attestation Responses Formulary – Inadequate Category/Class Count Supporting Documentation and Justification URR Template (also submitted in HIOS) Accreditation Template Administrative Data Template (2016 version) Plan ID Crosswalk Template (this also needs to be sent to CMS in XML to QHP [email protected])
QHP Benefit Standards and Product Offerings At least one silver plan and one gold plan must be offered in each carrier service area Plans may be offered with or without embedded pediatric dental Carriers may offer a maximum of five plans per metal tier within a service area (not including CSRs or Medicaid transition plans) Carriers are only required to submit a zero cost-share variation at the lowest metallic level for each product Standardized plans not required
Exchange Service Areas Nevada’s rating territories for 2017 are unchanged QHP and SADP service areas must equal one or more rating territories Only off-Exchange plan service areas may use partial counties
Quality Improvement Strategy (QIS) QHP issuers (not applicable for SADPs) who offered coverage in a marketplace two consecutive years (2014 and 2015), and who had a minimum enrollment of 500 enrollees must submit a QIS for implementation for plan coverage year 2017. https:// www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instru ments/QualityInitiativesGenInfo/Downloads/QIS-Technical-Guidance -and-User-Guide.pdf https:// www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instru ments/QualityInitiativesGenInfo/Downloads/QIS-Implementation-Pla n-and-Progress-Report-Form.pdf
Meaningfully Different Plan Designs Each qualified health plan must be meaningfully different in terms of either: - Metal level; Service area; Plan type; Premium and cost-sharing; Provider network; Covered benefits; or Formulary structure The Exchange will be utilizing the CMS Meaningful Difference Tool to identify redundant plan offerings
Discriminatory Benefit Design Examples Attempts to circumvent coverage of medically necessary benefits by labeling the benefit as a “pediatric service,” thereby excluding adults Refusal to cover a single-tablet drug regimen or extended-release product that is customarily prescribed and is just as effective as a multi-tablet regimen, absent an appropriate reason for such refusal Placing most or all drugs that treat a specific condition on the highest cost tiers, in particular: - Rheumatoid arthritis - Diabetes - Bipolar disorders - Schizophrenia
Rating and Premium Standards Rates must be the same for a plan inside and outside the Exchange Rates must be set for an entire benefit year, or for the SHOP, plan year Quarterly rate changes for SHOP plans are allowed, but must be submitted to the DOI at least four months prior to the proposed effective date Carriers must segregate funds: - Allocable to APTC - Allocable to individual - Federal funds cannot be used for elective abortions
2017 SADP Certification
SADP Certification Process SADP application in the form of a SERFF binder is required by 5/2 for plans on and off the Exchange The binder should only contain validated plan management templates and the Plan ID Crosswalk Template Carriers will not submit applications into HIOS Attestations and other supporting documentation will be collected from on Exchange carriers following final data transfer to CMS in August A SADP Issuer Agreement for the 2017 benefit year will need to be signed at the end of the certification process for plans on the Exchange
Certification Standards That Do Not Apply to SADPs Accreditation Cost-sharing Reduction Plan Variations Unified Rate Review Template Meaningful Difference Patient Safety Quality Reporting Prescription Drugs
SADP Timeline Key Dates 5/2 5/4 5/20 6/1 6/15 6/20 6/24 7/8 8/12 8/17 11/1 All QHP rate, form and binder filings due in SERFF 1st SERFF data transfer to CMS Correction notices sent to carriers via SERFF Revised data submitted to SERFF Correction notices sent to carriers Revised data submitted to SERFF Second SERFF data transfer to CMS Correction notices sent to carriers via SERFF Final date for carriers to resubmit data Final data transfer from SERFF to CMS Open enrollment
SADP Binders The following SERFF Plan Management Templates are required for certification, on and off the Exchange: – – – – – – – Plans and Benefits Template Rates Table Template Business Rules Template Service Area Template Network Template ECP/Network Adequacy Template Administrative Data Template (use 2016 version, add in supporting documents) All templates must be validated and submitted within a SERFF Binder Plan ID Crosswalk Template is required for on Exchange SADPs Attestations and other supporting documents will be collected at a later date
Plans and Benefits Template Only the built-in broad benefit categories should be used - No benefits may be added to a Benefits Package tab using the “Add Benefit” macro After pressing the “Refresh EHB Data” button, the following benefit categories auto populate and must remain “Covered”: – – – – Dental Check-Up for Children Basic Dental Care – Child Orthodontia – Child Major Dental Care – Child
Plans and Benefits Template If adult benefits are included in the plans, the following benefits must be changed to “Covered” with an EHB Variance Reason of “Not EHB” (was changed from Above EHB) : – – – – Routine Dental Services – Adult Basic Dental Care – Adult Orthodontia – Adult Major Dental Care – Adult Accidental Dental is included on the template but does not have to be covered
Plans and Benefits Template Quantitative Limit on Service, Limit Quantity, Limit Unit, and Minimum Stay should be filled out according to the most typical/highest utilized benefit in each “Covered” benefit category All other limits or details of the services provided should be described in the Benefit Explanation field Consumers should be able to easily access this detail when viewing your Plan Brochure
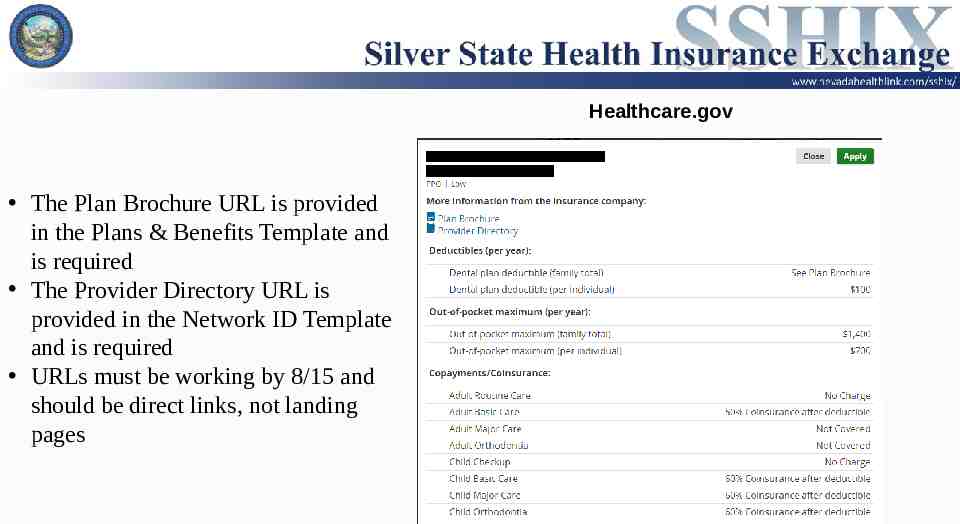
Healthcare.gov The Plan Brochure URL is provided in the Plans & Benefits Template and is required The Provider Directory URL is provided in the Network ID Template and is required URLs must be working by 8/15 and should be direct links, not landing pages
EHB Allocation for Pediatric Dental Portion of premium (dollar amount) that applies towards EHB Statewide average should be represented in template Cannot exceed premium for child-only plan Description of EHB Allocation form required to be signed by an actuary
Guaranteed vs. Estimated Rate Guaranteed – Carriers are bound to rates provided inside the Rates Table Template and the rating rules provided in the Business Rules Template Estimated – Consumers must contact carriers for final rate – This will be indicated on Plan Compare – Allows carriers to rate 19 and 20 year olds differently SHOP rates must be “Guaranteed”
Rates Table Template All SADPs in the individual and small group market must use individual age rating under the “Age” column Selecting “Family Option” to enter family tier rates is not permitted The rates for 19 and 20 year olds must be incorporated into the 0-20 age band
Business Rules Template Plans with “Estimated Rates” may adjust for rating factors not present in this template Plans with “Estimated Rates” may increase the maximum number of children rated on a contract, or remove the maximum altogether SHOP plans cannot exceed 3 dependents Required minimum relationships between primary and dependent: Spouse, Adopted Child, Foster Child, Ward, Stepson or Stepdaughter, Self, Child, Life Partner, Other Relationship
SADPs on Exchange Silver State Health Insurance Exchange Board requires purchase of pediatric dental for children Pediatric dental will be an optional purchase for children on HealthCare.gov Employers may purchase stand-alone dental directly on the SHOP without purchasing a QHP
SADP Plan Modification Stand-Alone Dental Plans are not subject to health benefit plan uniform modification rules HIOS Plan IDs can remain the same as plan year 2016, even with changes in cost-share Renewal with altered terms requires 60 day notice to policyholders
Annual Limits on Cost Sharing Stand-alone dental plans must have a maximum out-of-pocket limit applicable to pediatric essential health benefits that is no greater than 350 for one child or 700 for two or more children In the 2017 Payment Notice Final Rule, it finalized a new process which the annual limitation on cost sharing for SADPs would be increased over time. Any increase in the annual limitation would be implemented on plans in years beginning after 2017. Any increase would be based upon the percentage increase in the Consumer Price Index (CPI) for dental services and be made in 25 increments for coverage of one child. Only pediatric dental essential health benefits are subject to EHB rules, including meeting AV and out-of-pocket limit requirements
Pediatric Dental Essential Health Benefits All pediatric dental benefits within Nevada Check-Up as of March 31, 2012 must be covered. Benefits cannot have limitations which are more restrictive. Nevada Check-Up guidelines can be found at: http://doi.nv.gov/uploadedFiles/doinvgov/ public-documents/Healthcare-Reform/NV CheckUp Dental.pdf
Benefit Waiting Periods Waiting periods are generally not allowed for essential health benefits Carriers may require a reasonable waiting period for pediatric orthodontia Pediatric orthodontia waiting periods in excess of 12 months will not be approved Carriers with pediatric orthodontia waiting periods must prominently display disclosure language on page 1 of the schedule of benefits and, for on Exchange plans, include similar language within the Benefit Explanation field of the Plans and Benefits Template
Non-discrimination SADPs may not employ market practices or benefit designs that will have the effect of discouraging the enrollment of individuals with significant health needs. Type I services can only be subject to the deductible for the low AV plan.
Rates Rates must not be excessive, inadequate or unfairly discriminatory Rates are inadequate if they are clearly insufficient, together with the income from investments attributable to them, to sustain projected losses and expenses in the class of business to which they apply One rate is unfairly discriminatory in relation to another in the same class if it clearly fails to reflect equitably the differences in expected losses and expenses Individual SADP rates with expected expense ratios greater than 25% are presumed excessive under Nevada law Plans with adult dental benefits must develop rates for all ages based on the expected claim costs by age for the single plan benefit package
AV for Stand-Alone Dental SADP cannot use the AV calculator Must demonstrate that the plan offers essential health benefits at: – A low level of coverage – 70% – A high level of coverage – 85% Allows for a de minimis range of /- 2% Must be certified by an actuary
Certified Stand-Alone Dental Off the Exchange Satisfies “reasonable assurance” Allows a carrier to issue a health benefit plan without embedded pediatric dental if the carrier is reasonably assured certified standalone coverage has been obtained Nevada will consider self-attestation by an applicant to be “reasonable assurance” The health carrier must obtain “reasonable assurance” that the consumer has certified stand-alone coverage every year at renewal
Network Adequacy SADP counties must have at least: – One general dentist – One periodontist – One Oral surgeon – One orthodontist All providers must be within the specific travel standards established for each geographic area
Network Adequacy Distance and Time Standards Geographic Areas by County Urban Counties Carson City Clark Washoe Rural Counties Douglas Lyon Storey Frontier Counties Churchill Elko Esmeralda Euerka Humbolt Lander Lincoln Mineral Nye Perishing White Pine Maximum Travel Distance or Time 45 miles or 45 minutes 60 miles or 1 hour 100 miles or 2 hours
Essential Community Providers All SADPs are required to have a sufficient number and geographic distribution of ECPs An updated list of ECPs that provide dental services can be found at http:// www.cms.gov/cciio/programs-and-initiatives/health-insurance-marketplaces/ qhp.html Issuers must satisfy 30% ECP standards or submit supplemental ECP Response Form describing why they are unable to meet the threshold
2017 QHP Application Review Tools Automated data review tools used to check templates for data errors prior to submitting to CMS for review. Download toolkit at: http://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insuranc e-Marketplaces/qhp.html List of tools Data Integrity Tool – Identifies critical data errors within and across templates. Plan ID Crosswalk Tool –Checks to be sure Plan ID Crosswalk template has been completed correctly. Master Review Tool – Serves as a tool to generate data input file to other tools. Essential Community Provider Tool – Helps to verify the number of ECPs meets with requirements. Accommodates new data from the ECP/NA template.
List of Tools (cont) SADP Essential Community Providers Tool – Same as ECP tool but for SADPs. Meaningful Difference Tool – Compares all plans an issuer offers in a county to be sure there are not multiple plans that could appear identical to a consumer. Non-discrimination Tool – Looks at plans and runs through benefits to be sure no coverage is discriminatory. Cost Sharing Tool – Checks for cost sharing standards to be sure requirements are met. Category Class Drug Tool – Compares count of unique chemically distinct drugs in specific categories and classes against the benchmark. Non-discrimination Formulary Outlier Tool – Looks at plans where there are a high number of drugs that are subject to prior authorization in certain USP classes and flags them as outliers. Non-discrimination Clinical Appropriateness Tool – Analyzes availability of covered drugs associated with specific conditions to be sure that issuers are offering a sufficient type and number of drugs.
Data Integrity and Review Tool Expectations Carriers MUST use all the applicable tools provided by CMS to identify and resolve data errors prior to each submission. Carriers with data errors post-data lockdown that could have been identified and fixed through use of CMS tools incur the risk of not being certified
Plan Preview Module in the Health Insurance Oversight System (HIOS) Helps QHP and SADP carriers preview their own plan benefit displays for HealthCare.gov Confirm accurate plan data will be displayed on HealthCare.gov prior to data lock-down Helps states preview the plan benefit displays for all carriers in their state Closely mimics display consumers see on HealthCare.gov
Plan ID Crosswalk Template All carriers offering 2017 coverage must submit Plan ID Crosswalk template(s) to CMS and state – Applies to Stand-alone Dental Plans (SADPs) – Submit template in EXtensible Markup Language (XML) format to QHP [email protected] – Submit as supporting documentation within binder – Multi-State Plan (MSP) Program issuers complete template but follow a different submission process based on OPM instructions
Plan ID Crosswalk Template Submission Process Error Notices – CMS anticipates including crosswalk template errors with the broader correction notices for QHP certification reviews – Applies to Stand-alone Dental Plans (SADPs) State Authorization of the Plan ID Crosswalk Template – The DOI and Exchange will review template for compliance with Affordable Care Act market reforms such as uniform modification of coverage standards – Carriers will be notified by the DOI and Exchange if compliance issues are present – The Exchange will notify CMS when the Plan ID Crosswalk has been approved Carriers must use the Plan ID Crosswalk Review Tool prior to submission
SHOP- Small Business Health Options Program Qualifications Employees – must be between 1-50. Must offer coverage to all employees who work 30 hours or greater per week. Minimum participation rate is 75% for Nevada. Employers who enroll in SHOP coverage between November 15 and December 15 each year can offer SHOP coverage without meeting this percentage requirement. Must have an office or employee work site within the SHOP’s service area.
SHOP (Small Business Health Options Program) Employers offering coverage through SHOP can offer dental only plans without having to offer medical. Employee would have to enroll in dental plan before dependents could enroll (same as medical coverage). Dependent child-only plans will not be available in SHOP. Dependents of a qualified employee will be able to enroll only in the same medical and dental plans in which the qualified employee has enrolled.
SHOP (cont) Beginning in 2017 CMS will NOT support premiums based on Average Enrollee Premium Amounts
SHOP (cont) Online Renewals Two circumstances that are considered renewals: renewal of FF-SHOP participation AND the coverage that was previously offered, OR renewal of FF-SHOP participation but not renewing the previous coverage offered. Election period will begin when rate and plan information becomes available for the quarter in which coverage would end, but not more than two months before the date an enrollment must be submitted. Renewal of coverage. If a qualified employee enrolled in a QHP through the SHOP remains eligible for coverage, such employee will remain in the QHP selected the previous year unless— (1) The qualified employee terminates coverage from such QHP in accordance with standards identified in § 155.430; (2) The qualified employee enrolls in another QHP if such option exists; or (3) The QHP is no longer available to the qualified employee.
SHOP (cont) Employee Choice Employee Choice available to all qualified employers in all States. New to 2017 Employers will have a choice of three methods to make QHPs available to qualified employees (1) they can offer all QHPs from all actuarial values from one carrier (2) they can offer qualified employees a choice of all QHPs at a single level of coverage -- bronze, silver, gold, or platinum, or (3) they can offer a single QHP. Employers will also have the option to make available either (1) all SADPs at a single level of coverage – high or low, or (2) a single SADP.
SHOP (cont) Employee Group Size For plan years beginning on or after January 1, 2016, a small employer is defined as an employer who employed an average of at least one but not more than 50 full-time-equivalent employees on business days during the preceding calendar year and who employ at least 1 employee on the first day of the plan year. For groups going from large to small, provide documentation of number of employees.
CMS Account Manager Issuer’s primary point of contact for non-technical QHP and SADP issues related to the FFM. Clarifies issuers responsibilities and requirements for participation in the FFM (keep in mind NV is a SSBM state and sometimes different than most FFM states.) Coordinates resolution of cross-cutting issues. NON-TECHNICAL questions on the certification process.
Additional Resources for Issuers CMS Website: www.cms.gov – General information on the ACA and QHP application process. Link for specific plan management information: http://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Mark etplaces/qhp.html REGTAP website: www.regtap.info – Training and meeting materials. This is where you sign up for QHP related webinars. Also where presentation slides are available for download. You need to create an account to get access to REGTAP. CMS zONE: Contains a group especially for Issuers. Technical information is often stored here. This requires a special process in which to gain access.
Additional Resources for Issuers (cont) How to get CMS zONE access: EIDM CMS zONE Private Issuer Community
Additional Resources for Issuers (cont) ACA Exchange and Market standards: http://www.cms.gov/CCIIO/Resources/Regulations-and-Guidance/Do wnloads/508-CMS-9949-F-OFR-Version-5-16-14.pdf Code of Federal Regulations, Title 45, Parts 146,147, 148, 154, 156 Subpart B, and Part 158: http://www.ecfr.gov/cgi-bin/ECFR?page browse